Abstaining from sex does not enhance a man's fertility and may lower the chances of a successful conception for couples undergoing fertility treatment, according to new research presented at the annual conference of the European Society of Human Reproduction and Embryology in Madrid last week.
Fertility experts at the Soroka and Ben-Gurion Universities in Israel looked at sperm samples from around 6,000 men who had abstained from sex for up to two weeks, and found that the quality of the sperm declined after four days abstinence in men with normal sperm counts, and sooner in men with low sperm counts. The findings contradict current World Health Organisation guidelines, which recommend abstinence of between two and seven days before collecting semen for fertility treatment.
The researchers tested more than 7,200 semen samples from 6000 men who had abstained from sex for between two days and two weeks, 4,500 of which had normal sperm counts, while the remainder had a reduced sperm count. They found that in men with normal sperm counts, the proportion of healthy, strong-swimming (motile) sperm rose to a peak after four days of abstinence, before starting to drop. But in men with a low sperm count, the proportion of motile sperm fell after just two days, suggesting that any benefit to fertility gained by boosting the volume of semen following abstinence is cancelled out by a decline in sperm quality.
UK scientist Lyn Fraser said the results made good biological sense, adding that most men with low sperm counts have testes that are not producing sperm at full capacity and, when numbers are low, the quality is low. 'That means that if you abstain from sex for a long time, you?ll be ejaculating sperm that are old and necrotic', she explained.
'Our data challenge the role of abstinence in male infertility treatments' said team leader Elahu Levitas, saying that the results were most relevant for patients undergoing intrauterine insemination, for which the best quality sperm was needed. 'For these patients we recommend minimal abstinence ? ideally no more than two days' he advised.
[ Full Article ]
A lesbian couple are planning to use IVF to create a 'shared baby', the UK press has reported. Hayley Marlow and Vicky Hill want to have one of Ms Hill's eggs fertilised, using donor sperm, but to then implant any resulting embryo into Ms Marlow's womb. Ms Marlow would then be the birth mother, while Ms Hill would be the genetic mother of any child born.
The couple, who live in Oxfordshire, say they have consulted their GP about having a baby this way, but have not yet been referred to a specialist. Ms Marlow said they had got the idea because 'a lot of lesbians have children using male friends as sperm donors', but said they wanted to go one step further. 'We want a baby that has truly come from both of us and the only way to do that is by me carrying Vicky's baby', she said.
The two women are hoping to have the IVF procedure paid for by the National Health Service (NHS), but appreciate it will still cost them a lot of money. However, they want to do it because it will 'complete their family' - Ms Marlow already has a five-year old daughter from a previous heterosexual relationship. They say that any child they have will call Ms Hill 'mummy' and call Ms Marlow by her first name, Hayley. The couple will need the approval of their local NHS trust in order to proceed with the treatment, and the Department of Health has warned that its guidelines might not cover NHS IVF treatment in this way.
Pink Parents, a charity that supports gay couples raising families, said that it expected that most fertility clinics would be reluctant to perform the IVF procedure in this way, because the success rate is lower when transferring eggs from one woman to another. A spokesperson for Pink Parents said 'although rare, we are now receiving more requests for information on this type of pregnancy'.
A spokesman for the Human Fertilisation and Embryology Authority (HFEA), which regulates the provision of fertility treatment in the UK, said that there was no legal block on same-sex couples having fertility treatment. But, he continued, 'the couple would need to have a welfare of the child check to make sure they can provide a stable environment for the child'. He added 'If there were no father figure the clinician has to assess the kind of people who are going to be in the child's life who may be able to take that role'. A Department of Health spokesman said that it is 'extremely unlikely' that the couple will get their IVF on the NHS - explaining that couples must have tried for three years unsuccessfully to have a baby and have a 'defined cause of infertility' to be approved.
Air Quality in IVF laboratories is far more critical than in any other medical room.
Growing embryos can be very frustrating. Sometimes we just can't find any logical explanation why rates of success are dropping. Embryos are extremely sensitive. A deep concern should be involved when they are exposed to lab environment.
Click on image for full size.
Here are some points for concern:
VOC - is responsible for lack of success during the first years of any lab life."Off-gas" process along with a proper ventilation pattern could dramatically reduce the negative effects of VOC on embryo survival.
Ultra Violet Radiation: fluorescent lamps, the microscope lamp, sun light are all "contaminated"with UV light spectrum. UV is an excellent disinfectant, but we do not want to disinfect our embryos... Replacing the lamps with truly "UV free" lamps can solve this problem.
CO2 quality: compressed gases contain dangerous levels of organic (VOC) contamination. Use of pre –filtered CO2 VOC free, is essential.
Magnetic flux: Is probably responsible for many failures in the" In vitro fertilization" process. Modern equipment contains heavy electronic circuits. Electronic heaters and fans increase dramatically the magnetic flux in incubators and on laminar work stations. Studies showed that embryos in their first 24 hours are most sensitive to magnetic radiation from heated work surfaces and incubators. The DNA might be damaged at as low as 0.1 A/M magnetic field , while the magnetic flux inside incubators reaches levels as strong as 10 A/M. Until manufacturers will be more aware of that problem you can use a" Safety Box" that stops the magnetic flux and gives embryos a better chance to live.
Bio-Safe shields embryos against the strong magnetic flux found in most IVF equipment.
A major source of disease and contamination in hospitals and clinics lays in the air-conditioning systems and in the quality of air. Sore throat, red eyes, headaches, “lack of air syndrome" acquired diseases, are all part of the same problem.
Airborne concentrations of microbes and nano particles pose a hazard both to patients and staff. In many hospitals this source of contamination looks like a new, unfamiliar science. A simple air sample usually reveals contamination that has been associated with human health problems in indoor environments.
Base maintenance personnel have no regular access to provide periodic professional disease preventive maintenance (PM) on the hospital Heating, Ventilation and Air Conditioning (HVAC) systems.
Periodical examination and tests for "IVF CLINICS"
1. Air quality measurements
1.1. monitoring of air cleanliness according to ISO14644-1; 1.2. humidity and temperature patterns; 1.3. CO2 ppm in the airCO ppm in the air; 1.4. O2percentage in the air; 1.5. VOC levels in the air; 1.6. VOC levels in compressed CO2.
2. Measuring and evaluating the effective number of air changes in the room
2.1. evaluating the tightness factor; 2.2. measuring the number of air changes; 2.3. evaluating the air movement pattern in the room; 2.4. inspection of the AHU and filters, measuring the quality and efficiency of the HEPA filters; 2.5. measuring the differential pressure between the room and the surrounding relevant area.
3.Evaluating sterile qualities of the room and surroundings
3.1. evaluating airborne microorganisms in the room; 3.2. evaluating the cleanliness of the room and equipment (protein test and ATP test); 3.3. total microorganism count in samples taken from room surface and equipment; 3.4. evaluating the sterilization effectiveness of autoclave sterilizer and the way materials are being handled.
4.Physical environment hazards
4.1. monitoring the intensity of electromagnetic fields in the room; 4.2. monitoring the intensity of ultraviolet light; 4.3. monitoring the sound levels; 4.4. monitoring the quantity of positive ions in the air.
These series of tests, which last no more than a few hours, provide a clear and accuratepicture of the room and of the maintenance quality. There after one can determine what measures have to be taken in order to bring the room condition to an acceptable level. These series of tests determine the Room Grade according to the EN GMP.
We can learn a lot from monitoring the air for small particles.
When one has the proper measuring devices the monitoring is quick and gives a clear picture of the condition of a room. Following are the cases in which it is recommended to monitor particles in the air:
•In a new room: "particles’ counting" is required for an immediate feedback regarding the quality of the air system.
•During renovation and maintenance monitoring should be repeatedly done to make sure that the job is improving the air quality and not vice versa.
•During adjusting "air changes per hour", repeated "particles’counting" monitoring is to be done to regulate the optimum number of changes required.
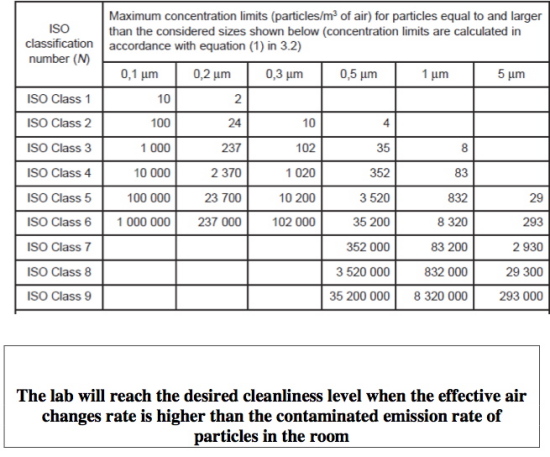
In the following table, the max. number of particles’ concentration according to ISO 14644-1, sorted by size, is shown. The common levels for hospitals are
Class 5: IVF laboratories, operating theaters - orthopedics (bones), open chest and cranium;
Class 6 : other operating theaters ;
Class 7 :intensive care units, sterile material storage rooms, air locks and sterile corridors and rooms.
The "Tightness Factor" (T.F) measurements for medical clean rooms
Keeping up the tightness factor dramatically improves the performance of medical clean rooms, improves the filtration process, the humidity and temperature control.
When tightness is poor, every opening of the door, little cracks or holes cause a purge of contaminated air into the room.
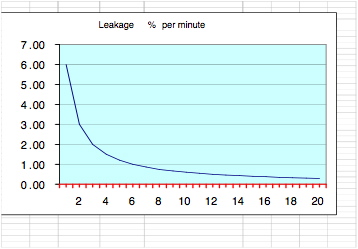
Standardtightnessfactoris reached in a room where pressure loss rate from 160 pascal to 60 pascal lasts more then 12 seconds . In this case the outside air penetration rate is smaller than 0.5 percent of the room volume in one minute and the filtration recovery system can cope with this amount of contamination and keep the room clean.
A clean room is a room that maintains a high tightness factor and the rate of filtration is higher than the rate of contamination per minute
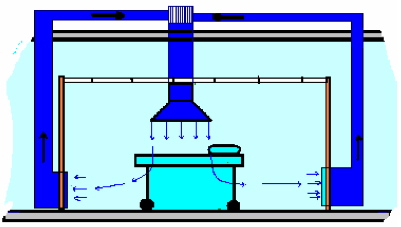
Air flow pattern
Clean air should reach the operation field in the shortest and most direct way. It should not cross through equipment or stuff. It should always move in the room from up to down. Any other flow pattern might cause cross contamination.
Positive Ion monitoring
Positive ions in the air are a common source of stuff and patients’ complaints of head ackes, feel of lack of air, sore throat and running eyes. The sources of ions are the ionization devices that are sometimes part of the air filtration systems.
Common causes of contamination in clinics
•The corridor that connects the operating rooms is not treated as a clean room, thus every door opening into the operating room causes a flow of contaminated air into the room;
•Medical and assistance stuff do not fulfill the hygiene instructions for operating rooms;
•Doors are left partially open during and after operations;
•Shuttting down the air-conditioning system ("because it is too cold") actually stops the filtering process;
•Servicing of the AHU and replacement of filters done by an unqualified technician and without strict regulations causes an enormous amount of dirt entering the room;
•Each room should have its own AHU. A common AHU might transfer contamination from one room to another. Furthermore, using a common AHU might influence the overpressure. Opening the door of one room brings down the overpressure from all other rooms;
•Without the ability to regularly monitor concentrations of particles in the air one cannot really determine when to change filters or if the room is a "clean" room.
•The source for fresh air is critical to the quality of the clean room. Hospitals have a hostile environment and contaminated air. The source for fresh air should be from the highest point possible and far from all obnoxious toxic contaminated discharges emitted by other departments.
•The HVAC system and tunnels are natural places for growing microorganism. They are the second most important cause for disease spread in hospitals. The first cause is the stuff itself. Decontamination measures should be done several times a year to reduce the risk.
Effective Decontamination methods for sterile rooms
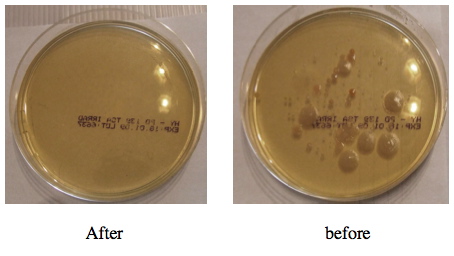
Ozone ( O3 ) in gas state is a highly effective decontamination means for the room surface and HVAC systems. The gas ozone reaches every little corner and crack that is unreachable or has been skipped by the cleaning team. In the attached photos you can see the results of air samples for bacteria presence in the air before and after the ozone treatment .
About the Author
Mr. Lehrmann has earned a nationwide reputation in Israel designing and implementing new methods and standards for CleanRooms
He holds an exclusive international patent for ‘Gas-tight Ventilation System’ and this, together with his many years of experience constructing gas-tight buildings, gained him the CTCB "PROFESSIONAL certification.
Mr. Lehmann applied his unique knowledge in the design and operation of ‘clean rooms’ to hospital operating theatres, IVF laboratories and isolation rooms throughout Israel. In fact he has set new standards in his approach to controlling and maintaining clean air – particularly with regard to the "Tightness Factor" parameter and the linkage between ‘Tightness and Air quality’.
As a result of his experience and many innovations, Mr. Lehrmann was invited to represent his work at the prestigious ‘Clean-Room Contamination Control Technology’ conference recently held at the world trade centre in Boston, MA, USA.
Dr Cong Fang is the associate director of the Reproductive Medicine Research Center of the Sixth Affiliated Hospital of Sun Yat-sen University as well as the director of the IVF–embryo transfer laboratory. She has been working on reproductive medicine as well as relevant research and education projects since 1998, from which she has accomplished rich experience in clinical management of infertility and relevant laboratory procedures. She was the first in China to convene researches on preimplantation genetic diagnosis for patients with chromosome translocations and to report the first successful pregnancy thereby.
The purpose of this study was to evaluate the effect of sequential embryo transfer in patients with repeated IVF failure. A retrospective matched case–control study was conducted and the outcomes of 213 patients with a history of repeated IVF–embryo transfer failure were analysed, of which 33 women underwent sequential embryo transfer on day 2 and day 3 (D2/D3 group), 66 women on day 3 and day 5 (D3/D5 group), 85 women underwent day-3 embryo transfer only (D3 control group) and 29 women underwent day-5 embryo transfer only (D5 control group) in the assisted reproduction centre of the Sixth Affiliated Hospital of Sun Yat-sen University from August 2010 to December 2011. The results showed that the clinical pregnancy rate of the D2/D3 group was higher than that of the D3 group (48.5% versus 22.4%, P=0.006) while the clinical pregnancy rates of the D3/D5 and D5 groups were not significantly different (50.9% versus 45.8%). Day-2 and day-3 sequential embryo transfer may improve the clinical outcomes for patients with repeated IVF–embryo transfer failures.
The clinical pregnancy rate following IVF–embryo transfer is usually 40–50% and can be as high as 60% in patients who are treated with IVF–embryo transfer for the first time (Margalioth et al., 2006). However, some patients experience repeated IVF–embryo transfer failures, and the success rate of subsequent IVF cycles in such patients is lower than the overall success rate. The possible reasons for failure include reduced endometrial receptivity, embryonic defects, immune factors, or multifactorial reasons (Lédée-Bataille et al., 2002). Improving the clinical pregnancy rate in these patients is a challenge faced by clinicians practising reproductive medicine and inadequate uterine receptivity is partly responsible for implantation failures. Thus, improving endometrial receptivity is essential to increase the IVF–embryo transfer success rate. In murine experiments, this study group has shown that embryos can induce better endometrial receptivity (Li et al., 2012).
In humans, sequential embryo transfer may be used to increase endometrial receptivity. Machtinger et al. (2006) reported that sequential transfer improves the pregnancy rate in patients with repeated IVF–embryo transfer failures. From 2010, sequential embryo transfer has been utilized for patients with repeated IVF failures in this study centre, and here are analysed the clinical outcomes of sequential and once-only embryo transfer to evaluate the effect of sequential embryo transfer.
Materials and methods
Patient selection criteria
Patients undergoing IVF–embryo transfer at the Sixth Affiliated Hospital of Sun Yat-sen University from August 2010 to December 2011 with three or more cycle failures were selected for the study. The inclusion criteria were age ⩽40 years, normal karyotype, normal immunological and thrombophilia screening, absence of endometrial abnormalities by hysteroscopy investigation and polycystic ovary syndrome, endometriosis, availability of 3 good-quality embryos on day 2 and 2 good-quality embryos on day 3.
During the study period, 165 women in the IVF unit underwent sequential transfer on day 2 and day 3 (D2/D3 group) or day 3 and day 5 (D3/D5 group), of which 33 met the necessary criteria for inclusion in the D2/D3 group and 66 met the inclusion criteria of the D3/D5 group. During the same period, 1310 women received day-3 transfer only, of which 85 women matched with the D2/D3 group in age, basal FSH concentration, cause of infertility, number of previous IVF cycles, number of oocytes retrieved and number of good-quality embryos on day 2 and were recruited as the D3 control group. Of the 115 women who had undergone day-5 transfer only during the same period, 29 cases matched with the D3/D5 group and met the inclusion criteria and so were recruited as the D5 control group.
This study was performed with patients’ consent and was approved by the ethical committee of the Sixth Affiliated hospital of Sun Yat-sen University (reference no. 2010013, approved 29 July 2010).
Ovarian stimulation and IVFD
The standard gonadotrophin-releasing hormone agonist long protocol (mid-luteal phase) was utilized. Briefly, 1.3mg triptorelin depot or 0.1mg triptorelin (IPSEN Pharma Biotech, France) was administered for down-regulation, and 100–300IU recombinant FSH (Puregon; Organon, Oss, Netherlands; or Gonal-F; Serono, Switzerland) was administered daily for ovarian stimulation. Follicle growth monitoring included serum oestradiol, progesterone and LH measurements and vaginal ultrasound investigation. When one follicle reached a diameter of 18mm or two follicles reached 17mm, 10,000IU of human chorionic gonadotrophin (Lizhu Pharmacy, Zhuhai, China) was administered and oocytes were retrieved 36h later. Routine IVF or intracytoplasmic sperm injection was performed 4h after oocyte retrieval, and the oocytes were checked for fertilization 16–18h later. Normal fertilization was indicated by the appearance of two pronuclei. Embryos were cultured in commercial sequential IVF medium (Quinn‘s Advantage Cleavage Medium; SAGE, Pasadena, CA, USA) for days 2 and 3.
Observation of the embryos
Embryos were observed at 48h (day 2) and 72h (day 3) after oocyte retrieval. The grading criteria for the embryos were as follows: grade 1, the size of the blastomeres was uniform, with no DNA fragmentation; grade 2, the blastomere size was slightly uneven with <20% DNA fragmentation; grade 3, the blastomere size was heterogeneous, or with 20–50% DNA fragmentation; and grade 4, >50% DNA fragmentation. The number and grade of the embryonic blastomeres were recorded. Good-quality embryos were defined as embryos containing 4 cells on day 2 (48h after oocyte retrieval) and 6 cells on day 3 (72h after oocyte retrieval) with a grade of 1–2.
Selection and transfer of embryos
In the D3 group, embryo transfer was carried out on day 3 after oocyte retrieval. Embryos with normal fertilization and graded as good-quality embryos on day 3 were selected for transfer. No more than three embryos were transferred. In the sequential D2/D3 group, one embryo was transferred on day 2, then remaining embryos were cultured to day 3 and one or two good-quality embryos were transferred. In the sequential D3/D5 group, one good-quality embryo was transferred on day 3, then the remaining good-quality embryos were placed in blastocyst culture medium (Quinn’s Advantage Blastocyst Medium; SAGE) and cultured until day 5. On day 5, one or two blastocysts were transferred. In the D5 group, all of the good-quality embryos were cultured to day 5, and one, two or three blastocysts were transferred. Luteal support was given with 20–40mg progesterone in oil (Xianju, Zhejiang, China) until 14 days after embryo transfer, and progesterone was maintained until 9–12weeks of gestation in pregnant patients.
Outcome measures
The primary outcome measures were the clinical pregnancy rate and implantation rate. The secondary outcome measure was the miscarriage rate. Pregnancy testing was performed 14days after embryo transfer. Ultrasound examination was performed at week 7 to assess the fetal sac number and the fetal heartbeat. Clinical pregnancy was defined as the presence of a fetal heart beat on ultrasound examination at 7weeks of pregnancy. The implantation rate was defined as the number of gestational sacs seen on the ultrasound divided by the total number of embryos/blastocysts transferred. Spontaneous miscarriage was defined as a clinical pregnancy loss before 28weeks of gestation age (Chinese Medical Association of Obstetrics and Gynecology Society, 2007). Multiple pregnancy was defined as two or more gestational sacs observed on ultrasound.
Statistical analysis
The Statistical Package for Social Sciences (SPSS, Chicago, IL, USA) was applied for data analysis. Data were expressed as mean±SD unless stated otherwise. Chi-squared test was used to analyse categorical variables while Student‘s t-test was used for continuous variables. A P-value <0.05 was considered statistically significant.
Results
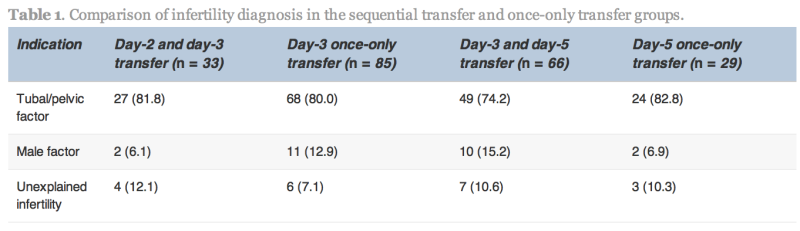
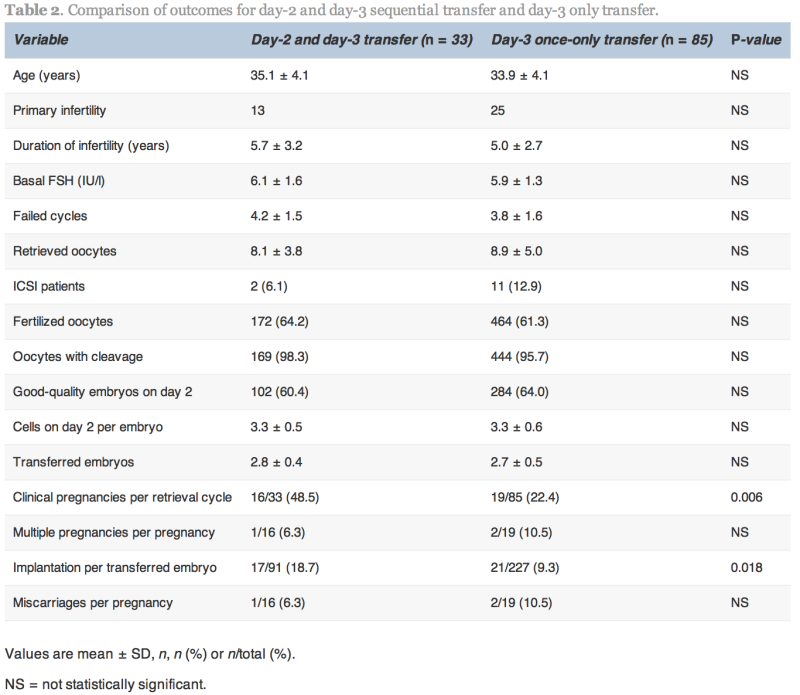
The indication for IVF, average age and duration of infertility in the sequential transfer and control groups were not significantly different (Table 1). No statistically significant differences existed between the groups with respect to the number of previous failed cycles, number of oocytes retrieved, fertilization rate, cleavage rate and percentage of good-quality embryos.
Values are n (%).
No statistically significant differences were found.
The clinical pregnancy and implantation rates in the D2/D3 group were significantly higher than the D3 group (48.5% versus 22.4%, P=0.006 and 18.7% versus 9.3%, P=0.018, respectively; Table 2). The multiple pregnancy rate was not significantly different between the two groups.
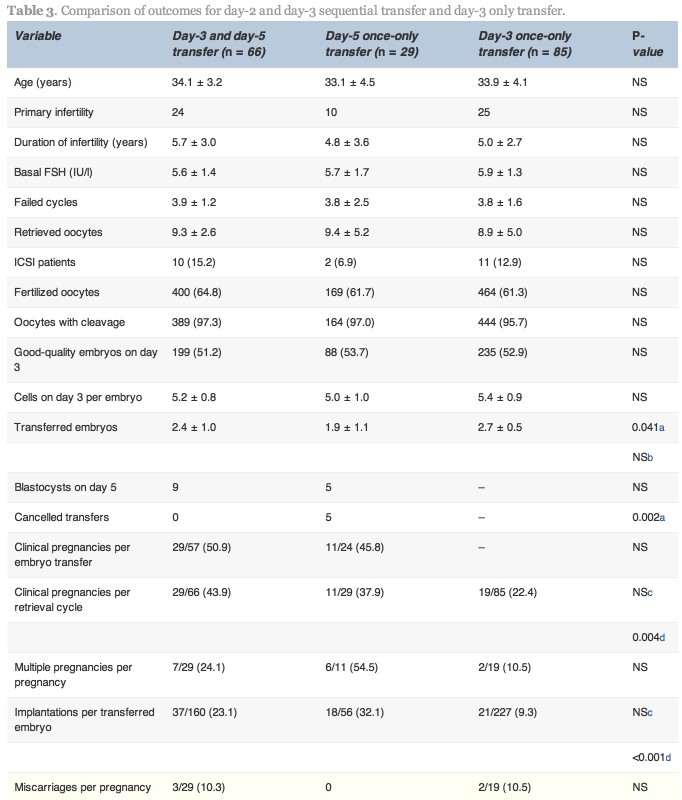
In the D3/D5 group, no blastocysts formed on day 5 in nine cases. In these nine cases, one patient conceived. In the 57 cases with both day-3 and day-5 transfer, 29 (50.9%) achieved pregnancy. In the D5 group, embryo transfer was cancelled because no blastocysts formed on day 5 in five cases, and in the 24 cases with blastocyst transfer, 11 (45.8%) achieved pregnancy.
No statistically significant differences existed between the D3/D5 group and the D5 group with respect to pregnancy and implantation rates; however, the cancellation rate was higher in the D5 group. Higher clinical pregnancy and implantation rates were obtained in the D3/D5 group than the D3 group (43.9% versus 22.4%, P=0.004 and 23.1% versus 9.3%, P < 0.001, respectively; Table 3).
Repeated IVF–embryo transfer failures may occur for a variety of reasons. The typical causes for repeated IVF–embryo transfer failures include reduced endometrial receptivity secondary to uterine cavity anomalies, an excessively thin endometrium, abnormal changes in the expression of adhesion molecules and embryonic developmental abnormalities, such as decreased embryo quality due to a poor culture environment and genetic factors. Some researchers have reported that two-thirds of IVF–embryo transfer failures are due to a lack of endometrial receptivity and one-third due to poor embryo quality (Achache and Revel, 2006). Therefore, at a state-of-the-art reproductive centre, assuming that the embryo culture environment is good, the key to improving the pregnancy rate is to improve endometrial receptivity.
This study’s findings suggest that day-2 and day-3 sequential transfer or day-3 and day-5 sequential transfer can improve the clinical pregnancy and implantation rates in patients with repeated IVF–embryo transfer failures. In the case of day-2 and day-3 sequential transfer, one embryo was transferred on day 2, which may induce an increase in endometrial receptivity, thereby creating a better endometrial environment for the second transfer on day 3. Studies have shown that co-culture of early-stage embryos with endometrial epithelium may increase the success rate of IVF–embryo transfer, especially in patients with repeated failures, indicating that the interaction between the embryo and the endometrium is important (Mercader et al., 2003,Tan et al., 2005, Spandorfer et al., 2006, Eyheremendy et al., 2010). At the same time, it has been shown that embryos can induce an increase in endometrial receptivity (Wakuda et al., 1999). Therefore, during sequential transfer, the embryo transferred on day 2 is co-cultured with the endometrium, which may improve the embryonic development potential and induce an increase in endometrial receptivity, thereby facilitating implantation of the sequentially transferred embryo. Also, mechanical stimulation of the endometrium has been reported to increase the pregnancy rate in patients with repeated IVF–embryo transfer failures (Barash et al., 2003, Zhou et al., 2008). During the first transfer on day 2, insertion of the catheter may be some kind of mechanical stimulation of the endometrium, inducing an increase in endometrial receptivity. Finally, increasing the likelihood of transferring embryos at the receptivity window of the endometrium by sequential transfer has been cited by some authors as another explanation for improved success rates in patients with repeated IVF/embryo transfer failures (Loutradis et al., 2004, Almog et al., 2008).
Transfer on day-3 and day-5 also improved the clinical pregnancy and implantation rates in patients with repeated IVF–embryo transfer failures compared with day-3 transfer, but no significant difference existed between the D3/D5 and D5 groups. It is well known that blastocyst transfer increases the likelihood for synchronized endometrial and embryonic development and endometrial receptivity, thus increasing the implantation rate. In two large-sample, controlled, prospective studies (Guerif et al., 2004, Levitas et al., 2004), blastocyst transfer was shown to significantly improve the implantation and live birth rates in patients with repeated IVF–embryo transfer failures; however, it is possible that no blastocyst forms during blastocyst culture so that no embryo can be transferred. Day-3 and day-5 transfer ensures transfer, on day 3, thereby reducing the effect of the high risk of cancellation of blastocyst transfer. In this study, the clinical pregnancy and implantation rates in the D3/D5 group were not superior to those in the D5 group, indicating that endometrial receptivity on day 5 is sufficient. Thus, the putative effects of the first transferred embryo and the mechanical stimulation by the first transfer have not been observed. However, it may be that statistical significance was not reached due to small sample sizes.
Concern remains regarding the risk of multiple pregnancy associated with sequential embryo transfer due to the high number of embryos transferred. In this study, the number of transferred embryos was similar between the D2/D3 and D3 groups; no difference existed in the incidence of multiple pregnancies. The D3/D5 group had a higher number of transferred embryos than the D5 group, but the incidence of multiple pregnancies was not different.
Ashkenazi et al. (2000) suggested that the second transfer procedure might have a deleterious influence, possibly related to infection or trauma, on the implantation of embryos transferred earlier. However, Tur-Kaspa et al. (1998) reported no significant differences in pregnancy rates with and without immediately repeated transfers. The current study concurs withTur-Kaspa et al. (1998) and shows that the second transfer had no adverse effect on the implantation process.
In addition, some researchers have reported that sequential transfer also improved the pregnancy rate of patients undergoing IVF–embryo transfer for the first time, and the beneficial effects of sequential embryo transfer on the implantation rate were also confirmed (Goto et al., 2003). Therefore, this method may be used not only in patients with repeated failures but also in poor-prognosis patients even in their first IVF–embryo transfer cycle in order to improve the pregnancy rate.
In conclusion, for patients with repeated IVF–embryo transfer failures, sequential transfer on day 2 and day 3 or on day 3 and day 5 may improve the clinical pregnancy rate in cases where no less than two good-quality embryos are available.
Acknowledgements
This study was supported by the National Natural Science Foundation of China (Grant no. 81070495) and the Natural Science Foundation of Guangdong Province (Grant no. 9151008901000018).
References
Achache H, Revel A. Endometrial receptivity markers, the journey to successful embryo implantation. Hum. Reprod. Update.2006;12:731–746 View In Article | MEDLINE | CrossRef
Almog B, Levin I, Wagman I, Kapustiansky R, Schwartz T, Mey-Raz N, et al. Interval double transfer improves treatment success in patients with repeated IVF/ET failures. J. Assist. Reprod. Genet. 2008;25:353–357 View In Article | CrossRef
Ashkenazi J, Yoeli R, Ovieto R, Shalev J, Ben-Rafael Z, Bar-Hava I. Double (consecutive) transfer of early embryos and blastocysts; alms and results. Fertil. Steril. 2000;74:936–940 View In Article | Abstract | Full Text | Full-Text PDF (63 KB) | CrossRef
Barash A, Dekel N, Fieldust S, Segal I, Schechtman E, Granot I. Local injury to the endometrium doubles the incidence of successful pregnancies in patients undergoing in vitro fertilization. Fertil. Steril. 2003;79:1317–1322 View In Article | Abstract | Full Text | Full-Text PDF (115 KB) | CrossRef
Chinese Medical Association of Obstetrics and Gynecology Society . Recommended guidelines for the diagnosis and treatment of preterm labor. Chin. J. Obstet. Gynecol. 2007;42:498–500 (in Chinese) View In Article
Eyheremendy V, Raffo FG, Papayannis M, Barnes J, Granados C, Blaquier J. Beneficial effect of autologous endometrial cellcoculture in patients with repeated implantation failure. Fertil. Steril. 2010;93:769–773 View In Article | Abstract | Full Text | Full-Text PDF (93 KB) | CrossRef
Goto S, Takebayashi K, Shiotani M, Fujiwara M, Hirose M, Noda Y. Effectiveness of 2-step (consecutive) embryo transfer. Comparison with cleavage-stage transfer. J. Reprod. Med. 2003;48:370–374 View In Article | MEDLINE
Guerif F, Bidault R, Gasnier O, Couet ML, Gervereau O, Lansac J, et al. Efficacy of blastocyst transfer after implantation failure.Reprod. Biomed. Online. 2004;9:630–636 View In Article | Abstract | Full-Text PDF (125 KB) | CrossRef
Lédée-Bataille N, Laprée-Delage G, Taupin JL, Dubanchet S, Frydman R, Chaouat G. Concentration of leukaemia inhibitory factor (LIF) in uterine flushing fluid is highly predictive of embryo implantation. Hum. Reprod. 2002;17:213–218 View In Article | MEDLINE | CrossRef
Levitas E, Lunenfeld E, Har-Vardi I, Albotiano S, Sonin Y, Hackmon-Ram R, et al. Blastocyst-stage embryo transfer in patients who failed to conceive in three or more day 2–3 embryo transfer cycles: a pro-spective, randomized study. Fertil. Steril.2004;81:567–571 View In Article | Abstract | Full Text | Full-Text PDF (72 KB) | CrossRef
Li TT, Fang C, Jia L, Yue CM. Mouse early integral embryo induces expression of endometrial integrin β3 and leukaemia-inhibitory factor, and improves uterine receptivity in mice. Chin. J. Pathophysiol. 2012;28:193–200(in Chinese) View In Article
Loutradis D, Drakakis P, Dallianidis K, Bletsa SR, Milingos S, Doumplis N, et al. A double embryo transfer on days 2 and 4 or 5 improves pregnancy outcome in patients with good embryos but repeated failures in IVF or ICSI. Clin. Exp. Obstet. Gynecol.2004;31:63–66 View In Article | MEDLINE
Machtinger R, Dor J, Margolin M, Levron J, Baum M, Ferber B, et al. Sequential transfer of day 3 embryos and blastocysts after previous IVF failures despite adequate ovarian response. Reprod. BioMed. Online. 2006;13:376–379 View In Article | Abstract | Full-Text PDF (167 KB) | CrossRef
Margalioth EJ, Ben-Chetrit A, Gal M, Eldar-Geva T. Investigation and treatment of repeated implantation failure following IVF–ET. Hum. Reprod. 2006;21:3036–3043 View In Article | MEDLINE | CrossRef
Mercader A, Garcia-Velasco JA, Escudero E, Remohí J, Pellicer A, Simón C. Clinical experience and perinatal outcome of blastocyst transfer after coculture of human embryos with human endometrial epithelial cells: a 5-year follow-up study.Fertil. Steril. 2003;80:1162–1168 View In Article | Abstract | Full Text | Full-Text PDF (104 KB) | CrossRef
Spandorfer SD, Soslow R, Clark R, Fasouliotis S, Davis OK, Rosenwaks Z. Histologic characteristics of the endometrium predicts success when utilizing autologous endometrial coculture in patients with IVF failure. J. Assist. Reprod. Genet. 2006;23:185–189 View In Article | MEDLINE | CrossRef
Tan Y, Tan D, He M, Gu M, Wang Z, Zeng G, et al. A model for implantation: coculture of blastocysts and uterine endometrium in mice. Biol. Reprod. 2005;72:556–561 View In Article | MEDLINE | CrossRef
Tur-Kaspa I, Yuval Y, Bider D, Levron J, Shulman A, Dor J. Difficult or repeated sequential embryo transfers do not adversely affect in-vitro fertilization pregnancy rates or outcome. Hum. Reprod. 1998;13:2452–2455 View In Article | MEDLINE | CrossRef
Wakuda K, Takakura K, Nakanishi K, Kita N, Shi H, Hirose M, et al. Embryo-dependent induction of uterine receptivity in the mouse endometrium. J. Reprod. Fertil. 1999;115:315–324 View In Article | MEDLINE | CrossRef
Zhou L, Li R, Wang R, Huang HX, Zhong Kl. Local injury to the endometrium in controlled ovarian hyperstimulation cycles improves implantation rates. Fertil. Steril. 2008;89:1166–1176 View In Article | Abstract | Full Text | Full-Text PDF (378 KB) | CrossRef
The risk of having a child born with certain congenital problems may increase with the father's age, US and Danish researchers say. In a study of over 70,000 births, published online in the journal Human Reproduction, they report that the risk of Down syndrome and other conditions begins to increase in children fathered by men aged over 35. The results could be due to genetic mutations in sperm caused by biological or environmental factors, the researchers say.
It is known that the rate of genetic errors in a man's sperm-producing cells increases with age, and previous research has suggested a link between increased paternal age and certain genetic conditions. However, the strong association between older mothers and a raised risk of conditions such as Down syndrome has hampered efforts to investigate the impact of paternal age. In the latest study, the team looked at data from 71,937 firstborn babies born in Denmark between 1980 and 1996. All had mothers aged between 20-29 years, to reduce the potentially confounding effects of increased maternal age.
The researchers found that there was no overall increased risk of birth defects related to increasing paternal age. However, they did find a link between older fathers and a raised risk of certain conditions - including Down syndrome and some syndromes involving multiple body systems or limb malformations. Compared to younger men aged between 20-29 years, the incidence of Down syndrome increased by 15 per cent in men aged over 35, rising to 30-40 per cent in fathers over 40. In men over 50, the risk was around three times higher that of younger men.
Previous research has shown that 5-9 per cent of Down syndrome cases are caused by a chromosome abnormality (an extra copy of chromosome 21) inherited from the father. The scientists say their results suggest that a high paternal age - as well as a high maternal age - could be 'an indication for screening'. They conclude that 'advanced paternal age may be associated with an increased occurrence of some specific malformations, including Down syndrome'.
New research hints that whether a man has sons or daughters is influenced by his genes. The study, by Mr Correy Gellatly from Newcastle University, was published in the journal Evolutionary Biology last week.
Mr Gellatly looked at 927 family trees from Europe and North America, detailing over 556,387 people, dating back to 1600. He observed that a man with many brothers is more likely to have sons, while a man with many sisters is likely to have more daughters. This effect was not seen in women.
The sex of a baby is determined by its father's sperm, an 'X' sperm (after the version of the sex chromosome it carries) makes a girl and a 'Y' sperm a boy. Mr Gellatly hypothesises that there is a gene, only active in males but a version of which is inherited from both parents, which determines the ratio of X and Y sperm a man produces.
He also suggests such a gene could explain the increase in baby boys being born after World War I. Mr Gellatly explains that the odds were in favour of men with more sons seeing a son return from the war. This would mean such men were likely to have sons, a trait inherited from their father. In contrast men with more daughters may have lost their only sons in the war, and those sons would have been more likely to father girls.
Other explanations have been proposed as to why the birth rate is not 50:50 in certain couples. It has been suggested that the sex of a baby could be influenced by differences in the time in a woman's monthly cycle sex happens, or the amount of time sperm spends in the testicles. Mr Galletly's study indicates there is a genetic component.
He says the net effect of such a gene is to balance out the population: 'If there are too many males in the population, for example, females will more easily find a mate, so men who have more daughters will pass on more of their genes, causing more females to be born in subsequent generations.'
The SCSA® test assesses DNA fragmentation using established methods that are supported by 25 years of research published in peer reviewed journals. These and ongoing studies indicate that sperm with elevated DNA fragmentation, as measured by the SCSA® test, have a lower probability of supporting a successful pregnancy.
The severity of male factors should be assessed prior to determining the appropriate treatment of couples presenting with infertility. The most common screening for male factors in the infertility evaluation is conventional semen analysis, which measures basic parameters including sperm concentration, motility and morphology. Severe and irreversible male factors are often treated successfully with intracytoplasmic sperm injection (ICSI) by injecting individual sperm into the egg cytoplasm.
ICSI bypasses all requirements of normal sperm motility and sperm/oocyte oolemma interaction. The only requirement for fertilization and early embryonic development is oocyte activation and adequate DNA integrity. Thus, a test of DNA integrity is very helpful in deciding which couple would most likely benefit from ICSI and which might be advised to consider other options such as donor insemination due to decreased odds for pregnancy with the male partner's sperm. Table I lists conditions when DNA fragmentation testing could potentially benefit a couple.
The Sperm Chromatin Structure Assay (SCSA®) test measures the percent of sperm in a semen sample that has fragmented DNA as well as the extent of DNA fragmentation. In the SCSA® test, sperm with very low levels of fragmentation fluoresce green, while sperm with moderate to high levels of fragmentation fluoresce red. The flow cytometer measures the ratio of red to green fluorescence in each of 5000 sperm. The percent of sperm with DNA fragmentation (red fluorescence) is expressed as the DNA Fragmentation Index (DFI; Evenson et al 2002).
The SCSA® test is a rapid, consistent, statistically robust test providing evidence for the relationship between sperm nuclear DNA fragmentation and function (Evenson et al 1991). DFI statistically derived thresholds of 0-15%, 16-29%, and >30% correlate with high, moderate, and low in vivo fertility potential, respectively (Evenson et al 1999). Specifically, if the DFI is >30%, there is a significantly greater risk for infertility (Evenson et al 1999, Evenson et al 2002, Spano et al 2002).
A preliminary study of in vitro fertility found a similar DFI threshold (>27%) to be predictive of a negative pregnancy outcome following ART (conventional in vitro fertilization and ICSI; Larson et al 2000). Larger subsequent studies including hundreds of infertile couples have validated that a man with >30% DFI has a significantly greater risk for infertility even with ART. Although this risk is influenced by a myriad of potential sources (maternal age, clinical techniques, etc.), exceeding this DFI threshold appears to decrease pregnancy rates by 50% upwards to 100% in some studies (Larson et al 2002a, Selah et al 2002, Virro et al, submitted).
SCSA® test parameters are weakly correlated with conventional examinations of sperm concentration, motility, and morphology (Evenson et al 1991, 1999). Semen samples with normal conventional parameters may have very poor DNA quality that contributes to infertility. Therefore, the SCSA® test offers additional clinical information not provided by conventional semen analysis alone.
Twelve couples with multiple failed ART cycles and no known male factors progressed to therapeutic donor insemination following discussion of their abnormal SCSA® test results (>30%). Nine of these couples conceived within 3 cycles of donor insemination after years of infertility (Virro et al, submitted). Insight into DNA integrity provided by the SCSA® test appears to offer an explanation for these previous failures.
Age (Evenson et al 2002a, Spano et al, 1998), long periods of abstinence (Spano et al, 1998), high fever (Evenson et al, 2000), and leukocytospermia (Alvarez et al, 2002) appear to be related to a significant increase in sperm DNA fragmentation. Data also show that exposure to environmental stresses, some prescription drugs (Evenson et al, 1999), pollutants (Selevan et al, 2000) or cigarette smoking (Spano et al, 1998; Potts et al, 1999) may have a detrimental effect on sperm DNA.
DNA fragmentation by the SCSA® test reflects the quality of sperm that have just undergone maturation in the male reproductive tract. While an excellent-quality sample is likely reflective of previous and future quality, poor DNA quality may be transient due to high fever, medications, physical or mental stress, or other unidentified conditions. Therefore, if SCSA® test results are poor, it is necessary to question the patient as to whether he has been exposed to conditions that may negatively affect sperm quality, correct these conditions if possible, and repeat the SCSA® test in 2 to 3 months.
The SCSA® test is a rapid, sensitive, unbiased, quantitative assessment of sperm DNA fragmentation that independently predicts natural and in vitro infertility. This prognostic information provides a significant medical, emotional, and financial benefit to couples considering ART, donor sperm or adoption.
Table I. Conditions Indicating SCSA® Testing
Unexplained Infertility
Persistent Infertility after Treatment of Female
Recurrent Miscarriage
Prior to Assisted Reproductive Technologies
Cancer in Male: Before and after Treatment
Abnormal Semen Analysis
Advancing Male Age (> 50 years)
References
Alvarez, JG, Sharma RK, Ollero M, Saleh RA, Lopez MC, Thomas AJ, Evenson DP, Agarwal AA. (2002) Increased DNA damage in sperm from leukocytospermic semen samples as determined by the sperm chromatin structure assay. Fertility and Sterility 78;319-329.
Evenson DP, Larson KL, Jost LK. (2002) The sperm chromatin structure assay (SCSA®): clinical use for detecting sperm DNA fragmentation related to male infertility and comparisons with other techniques. Andrology Lab Corner. Journal of Andrology 23;25-43.
Evenson D, Larson K, Jost L, Virro M, DeJonge C, Brannian J. (2002a) Relationship between age of man, sperm DNA fragmentation and infertility. April 2002, Seattle Washington. American Society of Andrology.
Evenson DP, Jost LK, Corzett M, Balhorn R. (2000) Effect of elevated body temperature on human sperm chromatin structure. Journal of Andrology 21;739-46.
Evenson DP, Jost LK, Marshall D, Zinaman MJ, Clegg E, Purvis K, De Angelis P, Claussen, OP. (1999) Utility of the sperm chromatin structure assay as a diagnostic tool in the human fertility clinic. Human Reproduction 14;1039-49.
Evenson, DP, Jost LK, Baer RK, Turner T, Schrader S. (1991) Individuality of DNA denaturation patterns in human sperm as measured by the sperm chromatin structure assay. Reproductive Toxicology 5;115-125.
Larson-Cook K, Brannian J, Hansen K, Jost L, Evenson D. (2002a) Relationship between assisted reproductive techniques (ART) outcomes and DNA fragmentation (DFI) as measured by the Sperm Chromatin Structure Assay (SCSA). American Society for Reproductive Medicine. Seattle Oct 12-17. #100777.
Larson KL, DeJonge CJ, Barnes AM, Jost LK, Evenson DP. (2000) Relationship of assisted reproductive technique (ART) outcomes with sperm chromatin integrity and maturity as measures by the sperm chromatin structure assay (SCSA). Human Reproduction 15;1717-1722.
Potts RJ, Newbury CJ, Smith G, Notarianni LJ, Jefferies TM. (1999) Sperm chromatin changes associated with male smoking. Mutation Research 423;103-11.
Saleh RA, Agarwal A, Nelson DR, Nada EA, El-Tonsy MH, Alvarez JG, Thomas AJ Jr, Sharma RK. (2002) Increased sperm nuclear DNA damage in normozoospermic infertile men: a prospective study. Fertility and Sterility 78(2):313-8.
Selevan SG, Borkovec L, Slott VL, Zudova Z, Rubes J, Evenson DP, Perreault SD. (2000) Semen quality and reproductive health of young Czech men exposed to seasonal air pollution. Environmental Health Perspectives 108;887-94.
Spano M, Bonde JP, Hjollund HI, Kolstad HA, Cordelli E, Leter G. (2002) Sperm chromatin damage impairs human fertility. The Danish First Pregnancy Planner Study Team. Fertility and Sterility 73;43-50.
Spano M, Kolstad AH, Larson SB, Cordelli E, Leter G, Giwercman A, Bonde JP. (1998) The applicability of the flow cytometric sperm chromatin structure assay in epidemiological studies. Human Reproduction 1998;2495-505.
Virro MR, Evenson DP. (submitted) Sperm Chromatin Structure Assay (SCSA®) related to blastocyst rate, pregnancy rate and spontaneous abortion in IVF and ICSI cycles. Fertility and Sterility.
Over the past 14 years, over half of the total number of embryos created for use in IVF in the UK have not been used, according to government statistics. Between 1991 and 2005, 1.2 million embryos were not used, from a total of more than two million embryos (2,137,924) created by specialists while assisting infertile couples in the UK to have babies.
In 2005, the live birth rate statistics improved to approximately 21.6 per cent, resulting in 11,262 children through IVF but still involving the creation of around 191,000 embryos. Lord Alton of Liverpool, an anti-abortion Independent peer, requested the data provided by the Department of Health's minister whilst challenging the permitted creation and uses of unwanted embryos particularly for research during recent parliamentary debates on the Human Fertilisation and Embryology (HFE) Bill 2007, a bill designed to revise and modernise its 1990 predecessor.
Lord Alton expressed surprise at the 'incredible rate' of unwanted embryos created in order to achieve successful pregnancies. The alarming data stirred evaluation of regulatory measures to reduce the number of extra IVF embryos destroyed. 'This is a rather unexpected aspect of IVF', Lord Alton admitted, and advocated embryonic-adoption programmes as a solution. Infertility organisations, including Infertility Network UK, felt there would be 'more scope for embryo donation' if encouraged. Bob Spink, the Conservative MP, turned to the medical community to address its high levels of embryo destruction.
Lord Winston, a leading UK fertility expert, tempered the debate with a reminder that even nature is highly inefficient and 'pretty well all of us' have created embryos through unprotected intercourse that do not implant and develop. Many experts estimate that only half of naturally-conceived embryos successfully implant and women commonly discard microscopic unviable embryos without detection.
Unused embryos in clinics under UK law may by consent be discarded, frozen, donated to research or donated to other infertile couples. Specialists create multiple embryos to increase the efficacy of IVF, an invasive, emotionally-taxing and expensive procedure. Only approximately 20 per cent of these will be considered viable for implantation. The others are usually discarded within days of production. Generally two embryos are transferred to the mother to increase chances of successful implantation. Viable embryos are often frozen for future use and must be destroyed within ten years. A smaller number are donated to research - 82,955 of the 1.2 million. Embryo donation to infertile couples for adoption is rare and generally unpopular with donating and prospective parents who were initially motivated to endure medical intervention to have a biological child.
Last month the Human Fertilisation and Embryology Authority revised its guidance to recommend that clinicians implant only one embryo. The measure aims to reduce risky multiple-birth pregnancies and thereby encourage scientists to discover IVF methods that require fewer embryos. A December 2007 HFEA report revealed that 64 per cent of embryo research conducted in the UK is dedicated to understanding embryo development to improve fertility treatments. Embryo donation for research significantly contributes to further scientific understanding. Many supporters argue it should be encouraged as a more respectful disposal alternative for embryos than pouring them down a drain without contributing to medical progress.
In case you hadn't already noticed, a public consultation has been taking place in the UK over the past few months. Your views are being sought as to whether couples should be able to choose the sex of their prospective children.
When a woman is expecting a baby, someone is sure to ask her whether she wants a boy or a girl. Some people genuinely don't mind which sex their baby is, whilst others have a clear preference. That preference might be motivated by vague notions of what boys and girls are like; it might be borne of a desire to balance up a family dominated by one sex; or it might be caused by real social and economic pressures. It's clear that some people really do care what sex their child is going to be. But is it right to act on that preference?
The organisation carrying out the public consultation, the Human Fertilisation and Embryology Authority (HFEA), decided to launch an enquiry into social sex selection after news from the United States that American couples are now able to determine the sex of their baby before conception, by using a technique that sorts sperm according to the sex determining chromosome they carry. The technique isn't currently available in the United Kingdom. But if and when it is, how should we react?
Is it always wrong to choose the sex of one's child for reasons other than avoiding a serious genetic condition? What happens if a couple has two or more children of the same sex: should they be given special permission to sex select? And what about the effect of sex selection upon society; would it skew the sex ratios or lead to discrimination? Or might it offer a harmless option to those couples who feel strongly enough to act? To take part in the consultation, go to http://www.hfea.gov.uk/forPatients/Consultations/ where you can complete the online questionnaire or download the full consultation document.
If you miss the deadline to respond to the HFEA public consultation, you could come along to Progress Educational Trust's conference next week in London to take part in a public discussion on sex selection. We have a wide range of speakers and delegates, and it promises to be an interesting and lively discussion. You can visit http://www.progress.org.uk/events for the full programme. Please email Laura Riley at [email protected] if you would like to attend. Delegates can pay on the door as long as they register in advance.
[ Full Article ]













 3 good-quality embryos on day 2 and
3 good-quality embryos on day 2 and