

IVF NewsNews: Free IVF for most UK couples?
Dr Kirsty Horsey 30 August 2003
The UK's National Institute for Clinical Excellence (NICE) has published the second draft of its proposed guidelines for infertility treatment provided by the National Health Service (NHS). It recommends that infertile couples meeting certain criteria should be offered up to three IVF attempts using fresh embryos, with the possibility of further treatment cycles using frozen embryos. The proposals could signal an end to the 'postcode lottery' provision of IVF, which at present varies greatly throughout the UK.
The guidance states that couples should be offered state-funded infertility treatment if the woman is between 23-39 years old, and if there is either a diagnosed cause of infertility, or at least three years of unexplained infertility. It also recommends that women under 23 may be offered treatment if the couple have an unequivocal need for IVF treatment, such as prior treatment for cancer, very poor semen quality or Fallopian tubal blockage. NICE also recommends that no more than two embryos per cycle of IVF treatment are transferred to the woman's womb, to reduce the risk of multiple pregnancy. The infertility patient support group CHILD has welcomed the production of the guidelines: 'The emotional impact of infertility on a couple's life is devastating, and finding themselves unable to access the treatment they need on the NHS causes further distress at an already very painful time in their lives' said spokeswoman Sheena Young. Fertility clinic director Simon Fishel also welcomed the proposals, saying that the UK has been 'the poor relation' in IVF provision compared to other western countries. But he also cautioned that it could take several years before the recommendations are implemented. The guidelines are now available on NICE's website (see link below), and people are invited to send their views until 22 September 2003, Anne-Toni Rodgers of NICE told the BBC. The final draft is due to be published in February 2004. [ Full Article ]  
Article: Current opinion on preimplantation genetic screening (PGS)
Joyce Harper 16 July 2009
Preimplantation genetic screening (PGS) for aneuploidy was first reported by Verlinsky et al (1995) and Munne et al (1995). Both of these initial studies analysed polar bodies. The aim of the technique is to help determine the best IVF embryo for transfer on the grounds of the polar body or embryo's chromosomes, by performing biopsy and analysis of the chromosomes using fluorescent in situ hybridisation (FISH). There have been hundreds of papers on the use of PGS. It is well known that for patients with advanced maternal age, there is an increased risk of chromosome abnormalities in the embryos they produce. Therefore this has been the main indication for PGS, but other indications include repeated IVF failure, repeated miscarriage (with normal karyotypes in the parents) and severe male factor infertility. As with many new technologies brought into the IVF clinic, there has been little evidence-based medicine to show that PGS increases delivery rates. At the late breaking news at the 2007 European Society of Human Reproduction and Embryology (ESHRE) annual meeting, Mastenbroek reported that their randomised controlled trial (RCT) on PGS showed that the treatment group had a lower delivery rate compared to the control group (Mastenbroek et al, 2007). Since then the debate about the validity of PGS has been rife. [ Full Article ]
News: IVF success rates from US show age is all important
Dr. Kirsty Horsey 13 January 2005
A report published by the US Centers for Disease Control and Prevention (CDC) shows that the younger a woman is when she uses assisted reproductive technology (ART), the more likely she is to become pregnant and have a live birth using her own eggs. The report defines ART as procedures in which both egg and sperm are handled in a laboratory, and says the majority of ART treatments its data include refers to IVF.
The CDC's annual report, released last week, used data for the year 2002 collected from 391 of the 428 fertility clinics in the US. The report, called '2002 Assisted Reproductive Technology Success Rates', showed that, in 2002, 45,751 live births were achieved from 115,392 ART procedures performed in the US. This was an increase from the previous year's figures, when there were 40,687 live births from 107,758 treatments. Overall, the per-cycle ART success rate in 2002 was 35 per cent, compared to 28 per cent in 1996. The 2002 data show that 37 per cent of women who undergo ART using their own, fresh eggs when they are below the age of 35, had a live birth. This is compared with 31 per cent of women aged between 35 and 37; 21 per cent of women aged between 38 and 40; 11 per cent of women aged between 41 and 42 and just four per cent for women older than 42. However, the report also showed that the age of the woman undergoing ART had 'little effect' on success rates if donated eggs were used. In 2002, the live birth rate for all ART procedures where donated eggs were used was 50 per cent, with the success rate varying only slightly between age groups. Victoria Wright, one of the authors of the CDC report, said that the data show that 'women in their 20s and early 30s who used ART had the most success with pregnancies, and single live births'. But, she added, 'success rates declined steadily once a woman reached her mid-30s'. She said the figures should act as 'a reminder that age remains a primary factor with respect to pregnancy success, and younger women have greater success than older women, even with technology'. [ Full Article ]
News: New rules for gay sperm donors to be introduced in US
Dr. Kirsty Horsey 12 May 2005
The US Food and Drug Administration (FDA) is introducing new rules about who can donate sperm. Men that have had homosexual sex within the five years prior to them wanting to make an anonymous sperm donation will be prevented from doing so, as the FDA says that gay men are collectively more likely to be HIV-positive than other men. However, men who have had male sexual partners within the past five years would not be prevented from donating sperm to a friend or family member. Critics accuse the FDA of stigmatising gay men rather than putting in place a screening process that focuses on high-risk sexual behaviour by any potential donors, gay or straight. [ Full Article ]
News: 'Saviour sibling' born to Fletcher family
Dr. Kirsty Horsey 23 July 2005
A Belfast woman has given birth to the first 'saviour sibling' conceived in the UK: a baby girl who could help treat her seriously ill three-year-old brother. In September 2004, the Human Fertilisation and Embryology Authority (HFEA) granted Joe and Julie Fletcher permission to have a tissue-matched baby to help treat Joshua, who has an incurable blood disorder. Following successful treatment at the Assisted Reproduction and Gynaecology Centre in London, Mrs Fletcher gave birth to daughter Jodie on 14 July. [ Full Article ]
Announcement: Graduate Programs in Reproductive Sciences and Reproductive Laboratory Science
Doris J. Baker, Ph.D., HCLD(ABB), MT(ASCP) 17 February 2010
The University of Kentucky now offers three graduate degree options in the Reproductive Sciences and Reproductive Laboratory Science, including a: 1) multidisciplinary Ph.D. in Reproductive Sciences; 2) master’s degree in Reproductive Laboratory Science; and 3) a Graduate Certificate in Reproductive Laboratory Science. Please refer to: http://www.mc.uky.edu/healthsciences/academic/index.html for complete information, including program requirements, curricula, course schedules, and procedures for application.
The Ph.D. is multidisciplinary in that coursework is completed in both the College of Medicine’s Interdisciplinary Biomedical Sciences curriculum and the College of Health Science’s Reproductive Sciences program, as well as other UK departments (e.g. statistics). The program is unique in that students have the option of completing the clinical curriculum in embryology/andrology as they progress through the basic science curriculum and complete dissertation research. Students may complete research in the laboratory of a faculty member, who is an active member of the University of Kentucky Reproductive Sciences Center, which is currently moving through the University approval process. It is anticipated that the university-wide Center will receive final approval in spring/summer, 2010. A limited number of competitive fellowships are available for qualified Ph.D. students.
The Master of Science is now a one-calendar-year curriculum (August-July). Although the Graduate Certificate is available to qualified individuals holding a B.S. in science or medical laboratory science, the certificate is intended for individuals already holding an advanced degree. Scholarships for the M.S. are limited and highly competitive.
Students enrolled in the clinical curriculum (M.S., Graduate Certificate, and Ph.D. with clinical option) complete practica at assisted reproductive technology centers throughout the United States, with the possibility of international internships. All clinical faculty directing students, are appointed as clinical faculty by the University of Kentucky. ART practitioners throughout the U.S. also contribute to didactic and student laboratory instruction to ensure that the curriculum is current and in line with clinical practice.
Applications to both the Graduate School and the specific graduate program is required for the Ph.D., the M.S. and the Graduate Certificate. Refer to: http://www.gradschool.uky.edu/. This site will also direct you to funding that is available through the Graduate School.
The deadline for applications for U.S. citizens/residents is April 15, 2010.
Please feel free to contact me if you are interested in one of the graduate programs after reviewing the information on the websites.
Doris J. Baker, Ph.D., HCLD(ABB), MT(ASCP) Professor, Center of Excellence in Reproductive Sciences Director of Graduate Studies, Reproductive Sciences University of Kentucky 126E CTW Building 900 South Limestone Lexington, KY 40536-0200 Telephone: (859) 218-0854 Fax: (859) 323-8957 E-mail: [email protected] [ Full Article ]
Announcement: WHO laboratory manual for the examination and processing of human semen. Fifth Edition (2010)
World Health Organization 06 April 2010

In press. This publication will be for sale. OVERVIEWSemen analysis may be useful in both clinical and research settings, for investigating male fertility status as well as monitoring spermatogenesis during and following male fertility regulation and other interventions. This manual provides updated, standardized, evidence-based procedures and recommendations for laboratory managers, scientists and technicians to follow in examining human semen in a clinical or research setting. Detailed protocols for routine, optional and research tests are elaborated. The fifth edition includes new information on sperm preparation for clinical use or specialized assays and on cyropreservation, an expanded section on quality control in the semen analysis laboratory and evidence-based reference ranges and reference limits for various semen characteristics. The methods described are intended to improve the quality of semen analysis and the comparability of results from different laboratories.
[ Full Article ]
Article: Improved development of mouse and human embryos using a tilting embryo culture system
RBM Online 28 March 2010

Koji Matsuura a,b, Nobuyoshi Hayashi c, Yuka Kuroda a,b, Chisato Takiue c, Rei Hirata c, Mami Takenami a, Yoko Aoi c, Nanako Yoshioka c, Toshihiro Habara c, Tetsunori Mukaida d, Keiji Naruse a,* a Cardiovascular Physiology, Graduate School of Medicine, Dentistry and Pharmaceutical Sciences, Okayama University, Okayama, Japan; b Research Core for Int erdisciplinary Sciences, Okayama University, Okayama, Japan; c Okayama Couples Clinic, Okayama, Japan; d Hiroshima HART Clinic, Hiroshima, Japan * Corresponding author. E-mail address: [email protected] (K Naruse).
Dr Keiji Naruse graduated from Nagoya University School of Medicine in 1988 (MD) and received his PhD in medicine from Nagoya University in 1992. He was an associate professor at Nagoya University from 1999 to 2005 and is currently a chairman and professor of Cardiovascular Physiology at Okayama University Graduate School of Medicine. He was a visiting professor at Harvard Medical School from 1998 to 2001. He has been working in the fields of mechanobiology of circulation, reproduction, and sensory systems. Abstract Mammalian embryos experience not only hormonal but also mechanical stimuli, such as shear stress, compression and friction force in the Fallopian tube before nidation. In order to apply mechanical stimuli to embryos in a conventional IVF culture system, the tilting embryo culture system (TECS) was developed. The observed embryo images from the TECS suggest that the velocities and shear stresses of TECS embryos are similar to those experienced in the oviduct. Use of TECS enhanced the development rate to the blas- tocyst stage and significantly increased the cell number of mouse blastocysts (P < 0.05). Although not statistically significant, human thawed embryos showed slight improvement in development to the blastocyst stage following culture in TECS compared with static controls. Rates of blastocyst formation following culture in TECS were significantly improved in low-quality embryos and those embryos cultured under suboptimal conditions (P < 0.05). The TECS is proposed as a promising approach to improve embryo development and blastocyst formation by exposing embryos to mechanical stimuli similar to those in the Fallopian tube. RBMOnline © 2009, Reproductive Healthcare Ltd. Published by Elsevier Ltd. All rights reserved. Declaration: Keiji Narusee launched the bio-venture company, Strex Inc., in 2003 and serves as a Chief Scientific Officer. The other authors report no financial or commercial conflicts of interest. KEYWORDS: blastocyst, embryo development, mechanical stimuli, shear stress, tilting embryo culture system Introduction Mammalian embryos are transported to the uterine cavity through the Fallopian tube during cell cleavage, blastomere and blastocyst development (Eddy and Pauerstein, 1980; Halbert et al., 1976). In conjunction with ciliated epithelium, the Fallopian tube acts as a peristaltic pump due to phasic contraction of the smooth muscle in the wall to transport the embryo (Lyons et al., 2006; Zervomanolakis et al., 2007). Based on the movement of cilia and the similar size between the tubal lumen of ampulla and isthmus (Table 1) and the diameter of the embryo (0.1 mm), fertilized oocytes may be subject to a mechanical influence from the Fallopian tube lumen, such as compression and shear stress from the tubal fluid. It is postulated that these mechanical actions in the Fallopian tube might play an important role in embryo development. However, conventional in-vitro static culture conditions do not mimic mechanical stimuli to embryos. Providing mechanical stimuli to developing embryos in-vitro, similar to that experienced in the Fallopian tube, may improve development. 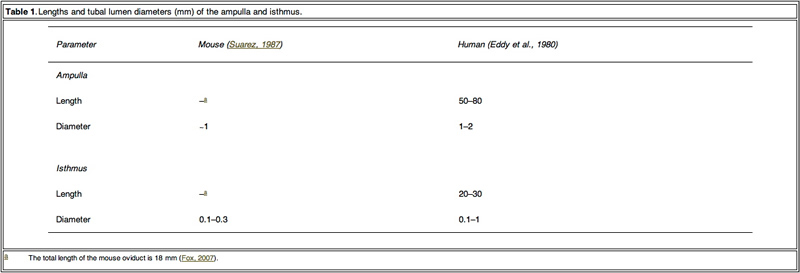 Table 1. Click on image for full size. From the 1980s, some groups reported in-vitro non-static culture results (Nagai et al., 1993; Staigmiller and Moor, 1984). However, these reports did not discuss the precise effect on embryo development from cleaved embryo to blastocyst. Recent papers have reported that a microfluidic dynamic embryo culture system with media flow improved mouse embryo development (Cabrera et al., 2006). The report proposed the importance of the physical/mechanical environment on embryo development. Because the systems are complex to handle, clinical application of the culture system is quite difficult. In addition to ease-of-use, another consideration regarding mechanical stimulation during embryo development is avoiding excess stress. Excess mechanical stimuli would damage embryos. It was found that shear stress over 1.2 dyn/cm2 caused lethality within 12 h for blastocysts (Xie et al., 2006). Over-handling of embryos, such as excess pipetting, caused elevation of phosphorylated stress- activated protein kinase and may cause rapid transient changes in hundreds of proteins and mRNA (Xie et al., 2007). In order to construct a dynamic culture system that can apply a mechanical stimulus and can be easily adapted to conventional static culture platforms, the tilting embryo culture system (TECS) was developed. Placing a conventional culture dish or plate on a tilted plate makes embryos in culture move along the bottom of the dish by gravity. Animal model experiments using TECS were first conducted, for the in-vitro culture of mouse 2-cell-stage embryos. A subsequent study using thawed human embryos cultured on TECS was also performed. Materials and methods Observation of embryo motion and shear stress calculation To estimate the shear stress applied to embryos, mouse embryo motion in the microdrop on the tilting plate of a prototype TECS was observed by objective lens (20x) attached to the bottom of the tilting TECS plate. To estimate the flow velocity of media in the microdrop, this study observed the motion of the microspheres (0.5–5 μm diameter) in the microdrop covered with mineral oil by tilting inverted microscope (Eclipse, Nicon, Tokyo, Japan), particularly focusing on the motion of microspheres at the centre of the bottom where embryos in the microdrop were moving. When the microscope was tilted, the particles moved in the same direction as the leaning microscope. The average particle velocities, which were considered as the velocity of the medium in the microdrop, were calculated. Under the holding the tilt and static conditions, Brownian motion of the particles was dominant. Images of moving embryos and microspheres were recorded by a charge-coupled device camera connected to a personal computer. The frame rate of the recording was 30 frames/s. The observed maximum velocity of the embryos and the velocity of the medium were VE and VM, respectively. The velocity to estimate maximum shear stress (VSS) was calculated from the difference between VE and VM. VSS =VE -VM The maximum shear stress applied to embryos during the tilting was calculated from the following equation: Shear stress = 6µrVSS =4µr2 = 6VSS dyn/cm2 where µ is the viscosity of the medium and r is the radius of the embryo. In an attempt to provide as accurate an estimate as possible regarding sheer stress experienced by embryos, this study attempted to determine the flow velocity of fluids using microspheres. The above equations are applicable in the flow condition. Generally, the effect of Brownian motion during flow can be neglected for the shear stress calculation. However, it would be difficult to determine accurate fluid velocity by particle image velocimetry. Although forces such as friction come into play with this approach, it provides a rough estimation for the final calculations. Embryo motion in extirpated mouse oviducts was observed as follows. Female ICR mice (8–12weeks old; Charles River Japan, Yokohama, Japan and Shimizu Laboratory Supplies, Kyoto, Japan) were injected with 5 IU pregnant mare’s serum gonadotrophin (Aska Pharmaceutical, Tokyo, Japan), followed by 5 IU human chorionic gonadotrophin (Aska Pharmaceutical) 48h later and mated with males. Successful mating was determined the following morning by the detection of a vaginal plug. Two days after the mating, the oviduct was extirpated with embryos and the oviduct was sandwiched between a cover slip and a glass slide to observe the embryo in the oviduct. The velocity of the embryo in extirpated mouse oviducts was calculated from the movie of the embryo motion. Animal use protocols were approved by Okayama University animal investigation committee. Specification and motion programmes of TECS TECS (Strex, Osaka, Japan) is an electrical device with a power cord that is designed to be used in a humidified incubator. This device consists of a control unit (Figure 1A, upper) and a motor unit with a tilting plate (Figure 1A, lower). Four-well chambers and/or dishes are set on the plate. The TECS motor unit is controlled and DC-powered by a cord connected to the control unit through an access hole in the incubator. If the incubator does not have an access hole, a flat-type cable extends tightly through the door of the incubator in order not to alter temperature, gas concentration and humidity inside the incubator. The motor unit is waterproof. The controller outside the incubator puts in the motion parameters.  Figure 1. Click on image for full size. A representative motion programme of TECS is shown in Figure 1B and C. The TECS can control the parameters of the uniform radial velocity (Vr), the maximum tilt angle (θr) and the holding time at the maximum tilt angle (Th). The tilting time (Tr) in seconds is calculated from 2θr/Vr. First, the plate is tilted to the positive maximum tilt angle (+θr) (M1). Second, the tilting plate is held for Th with no motion (M2). Third, the plate is tilted to the negative maximum tilt angle (−θr) (M3). Last, the tilting plate is held for Th with no motion (M4). The TECS motion cycle is summarized in Figure 1C. The cycle continues until the power is turned off. To apply conventional culture dishes/approaches to the TECS, spill out of the mineral oil should be prevented. The angles at which mineral oil begins to spill out are different according to the size of the dishes. The mouse embryo experiments used dishes of 35 mm diameter and maximum tilt of 20 degrees. However, in the human embryo study, the plate could not be tilted over 10 degrees due to the use of dishes of 60 mm diameter. The maximum tilt angle that caused mineral oil to spill out was surveyed and the limit of the maximum tilt angle was approximately 20 degrees in the microdrop setup. Furthermore, excess uniform radial velocity also induces spill out of the mineral oil. The minimum radial velocity at which the mineral oil spilt from the 35 mm dish was 240 degree/s when the maximum tilt angle was 20 degrees. The oil did not spill out when the tilt angle was 10 degrees. It is necessary to increase the maximum tilt angle and radial velocity in order to move embryos in the microdrop. However, this study set the maximum tilt angle and radial velocity so that they did not result in the spilling out of the mineral oil but still allowed the observation of embryo motion in the video rate recording. Thus, the maximum tilt angle was 10–20 degrees and the radial velocity was approximately 1 degree/s. Tilting mouse embryo culture Frozen 2-cell-stage embryos of ICR mouse (Arc Resources, Kumamoto, Japan) were thawed and cultured in 50 and 500 μl, respectively, of potassium simplex optimized embryo culture medium (Daiya Shiyaku, Tokyo, Japan). The culture medium was covered with mineral oil and incubated for 3 days in a humidified environment of 5% CO2 in air at 37°C. In the TECS group, the mouse embryos were cultured at a maximum tilt angle of 20 degrees with a holding time of 1 min. The plate was rotated at 1 degree/s to reach a total tilt of 20 degrees. To count cells in the mouse blastocyst, the cells were stained with Hochest 33342, as previously reported (Hardy et al., 1989; Mottla et al., 1995). The stained blastocysts were observed by confocal microscopy (FV-1000; Olympus, Tokyo, Japan) and a 3D image was constructed. Human embryo study The human embryo study used 3- to 11-cell-stage embryos frozen by the slow method 3 days after collection of the oocytes from May 2000 to December 2004 (Cohen et al., 1985) and extended the prospective study of 220 fertilized human embryos that were to be discarded with consent after pregnancy of patients. This study was approved by the ethics committee of the Okayama University Graduate School of Medicine. The frozen embryos were thawed with THAW-KIT 1 (Vitrolife, Gothenburg, Sweden) and the viability of the thawed embryos was approximately 80%. Once thawed, human embryos were cultured in a 20 ll microdrop of Global medium (LifeGlobal, Ontario, Canada) covered with mineral oil for 48 h. The thawed embryos with morphologically regular cleavage were divided so that there would be the same percentage of embryos with regular cleavage (33%) in both the TECS group and the control group. The viable cell number of the thawed human embryos was from three to 11. The dishes were placed on the tilting plate of TECS in a 50 l multi-gas incubator (ASTEC, Fukuoka, Japan). The thawed human embryos were cultured at a 10 degree tilt for 10 min. The radial velocity of the tilt was 1 degree/s (Vr). The blastocysts were morphologically evaluated according to the classification of Gardner et al. (2000). The cells in the human blastocyst were stained with Hochest 33342, the blastocysts were observed by confocal microscopy (FV-1000 Olympus, Tokyo, Japan) and a 3D image was constructed. Statistical analysis Chi-squared test and Student’s t-test were used to determine differences in the blastocyst development rate and in the number of cells in the blastocysts between the groups, respectively. A P-value < 0.05 was considered significant. ResultsObservation of embryos in motion by TECS and estimation of shear stress To obtain detailed information on the embryo motion, the blastomeres were observed on the TECS during tilting and holding. Figure 2 shows cropped images of the mouse embryos in motion. Between each 10 degree tilt (M1 and M3 in Figure 1B), the TECS plate was tilted at 1 degree/s. The motion of the medium was observed in M1 and M3 (Figure 1B). The embryo moved at a velocity of 1.5 mm/min on average (Figure 2A and B), which gave rise to shear stress of 7.0 x 10-3 dyn/cm2 at the bottom of the centre in the microdrop at a velocity of 0.1 mm/min. When the TECS plate was held at a 10 degree tilt (M2 and M4 in Figure 1B), the embryo slid at a velocity of 0.03 mm/min (Figure 2C, D), which gave rise to a shear stress of 1.5 · 10–4 dyn/cm2 in the medium, where the motion of medium at the centre of the bottom was neglected in the motion phases. These values are summarized in Table 2. 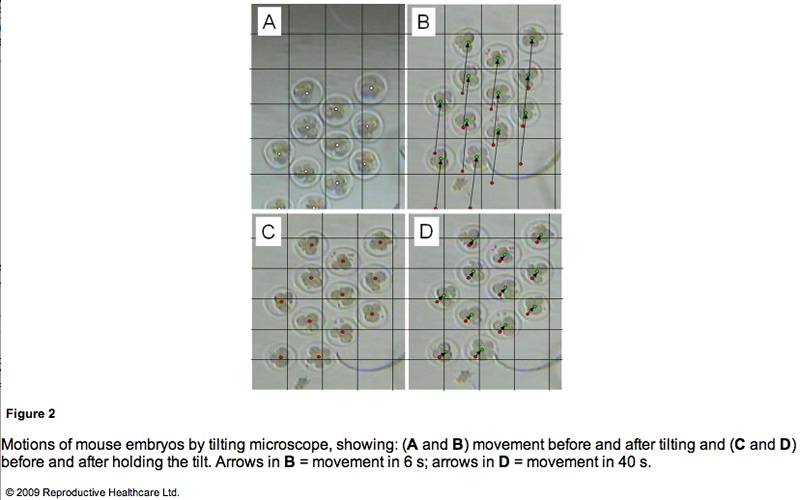 Figure 2. Click on image for full size. 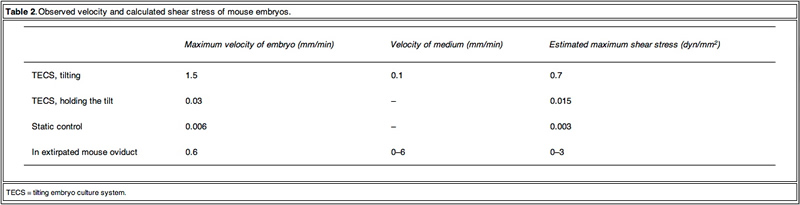 Table 2. Click on image for full size. Mouse embryo development Table 3 shows the blastocyst development rates from 2- cell-stage mouse embryos cultured under several conditions. As shown in Figure 3, the blastocyst development rate was 79% for 10 embryos in a 50 ll microdrop using the TECS, which was not significantly different to the static culture controls (75%). Because mouse blastocyst development rate is reported to be influenced by the number of embryos in the culture medium (Melin et al., 2009) and in order to enhance the statistical difference between TECS and control, the number of embryos in the microdrop were deduced and the medium volume-to-embryo ratio, which might simulate poor development condition and lead to low-quality human embryos, was increased. The blastocyst development rate for four–six embryos in a 50 ll microdrop was less than that of 10 embryos, although in this poor condition, TECS significantly improved the blastocyst development rate (TECS 59% (n = 145) versus control 46% (n = 151); P < 0.05). When 10 embryos were cultured in 500 ll medium, the blastocyst development rate decreased to 27% (n = 101) in the static control, whereas for those cultured in the TECS it was significantly higher (42% (n = 99); P < 0.05)). The number of cells in the blastocysts cultured using the TECS was (mean ± SEM) 77 ± 4 cells (n = 34), while that of the control was 66 ± 4 cells (n = 26), as shown in Figure 4. There was a significant difference in the average cell number between the two groups (P < 0.05). 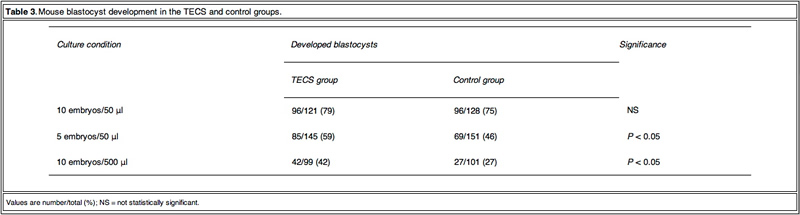 Table 3. Click on image for full size. 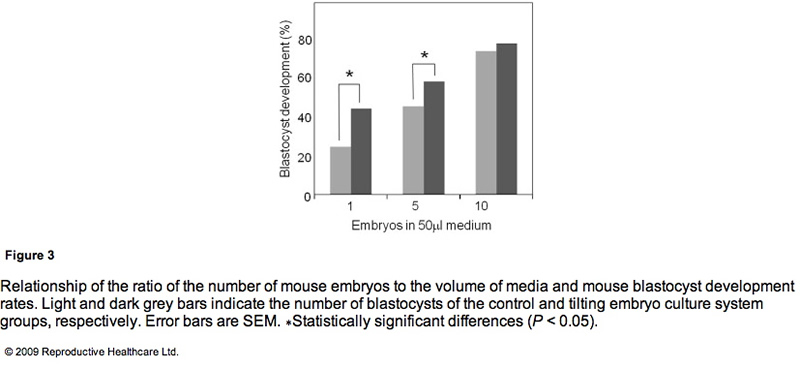 Figure 3. Click on image for full size.  Figure 4. Click on image for full size. Human embryo development As TECS enhanced blastocyst development rate in mouse embryos, experiments were then conducted on thawed human embryos. The development rates to the blastocyst stage of the TECS and control groups were 53% and 45%, respectively (Table 4).  Table 4. Click on image for full size. Due to the insufficient sample number of thawed human embryos, the study investigated the cell number of the developed blastocysts instead of the blastocyst development rate. Figure 5 shows the comparison of average cell numbers in human blastocysts developed by the TECS and control groups. The mean cell number of developed blastocysts at day 5 by the TECS was 43±3 cells (n=24), while that of the control was 34 ± 3 cells (n = 18). There was a significant difference in the average cell number between the two groups (P < 0.05). 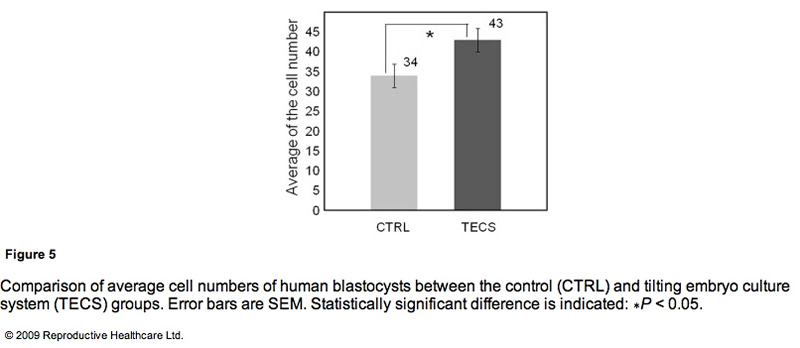 Figure 5. Click on image for full size. Discussion The Fallopian tube is a multifunctional organ, involved in receiving ovulated oocytes, providing a suitable environment for fertilization and early development and transporting embryos to the uterus. Here, light is shed on the mechanical properties of the Fallopian tube that might influence early development of embryos during culture. Early studies showed that the Fallopian tube is a mechanically active organ and may have influence on development due to: (i) shear stress by a tubal fluid flow; (ii) compression by peristaltic tubal wall movement; (iii) buoyancy; and (iv) kinetic friction force between embryo and cilia. Punctuated velocities of maxima from 0.39 to 1.8 mm/min have been observed in rat oviducts for microspheres emulating the size of embryos (Xie et al., 2006). Inappropriate culture conditions could be detrimental. Indeed, embryos sense shear stress and development is compromised (Xie et al., 2006, Xie et al., 2007). Because shear stress is a function of the velocity of the embryo and the flow and because the contribution is important, it is propose that the velocity of embryos should be made similar to those in the oviduct. Similarity in the velocities of the mouse embryos was found but those of other species were not observed. The velocities in-vivo and ex-vivo should be investigated for optimization. The observed velocity of mouse embryos on a TECS culture plate was of a similar order to those proposed in the oviduct. The embryo motion in the microdrops on the TECS plate relates directly to the plate motion. The observed embryo images on the TECS plate suggest that the velocities and shear stresses of embryos (Table 2) in the TECS plate and the oviduct are similar. This comparative experiment suggests that the TECS can apply physiological mechanical stimuli to mouse embryos. In the case of human embryos, the embryo velocity in the microdrop on the TECS plate was the same order (approximately 1 mm/min) as those of mouse embryos and below 1.2 dyn/cm2. Therefore, the TECS could apply physiological stimuli without an excess amount of shear stress that might cause damage to the embryos. Furthermore, the detrimental or beneficial shear stress would be different at each developmental stage and future experiments will address this. Embryo motion in fluid is affected not only by species differences but also the environment of the embryos. For example, when cumulus cells are coated with zona, embryos with the cells stick on the bottom of the dish. To optimize the parameters (θr and Vr) for each embryo condition, the relationship between the motions in fluid and physical characteristics of embryos (such as density, dimension and zona surface structure) should be considered. The TECS significantly improved development in low-quality human embryos and suboptimal culture conditions in mouse embryos. The significance of the improvement by the TECS was dependent on the number of mouse embryos in the medium. As mentioned in the results, the blastocyst development rate significantly improved in the case of four–six mouse embryos in the microdrop. In the case of 10 embryos in the microdrop, blastocyst development rates of the TECS and control groups were 75% and 79%, respectively, and the difference was not significant. A higher number of embryos in the medium can improve the blastocyst development rate. According to previous reports that the concentration and production of autocrine and/or paracrine factors enhance mouse embryo development (Contramaestre et al., 2008, Kawamura et al., 2005), a higher number of embryos in the medium can improve the blastocyst development rate. The results in Figure 3 demonstrate that blastocyst development rate was significantly improved by the TECS when using a lower ratio of mouse embryo to media volume. This may be due to diffusion of growth factors and/or waste products, which would be facilitated by the TECS motion in the mouse embryo culture. However, mechanical stimuli could also be beneficial. Indeed, in bone and endothelial cells, down-stream transcription factors in the nucleus have been shown to be activated by mechanical stimuli, such as shear stress and mechanotransduction, and gene transcription and DNA syntheses were also activated (Wang and Thampatty, 2006). Due to the enhancement of cell division induced by these activations, cell numbers would be increased without apoptosis. The results demonstrated that the cell numbers of the mouse and human blastocysts cultured in the TECS were greater than those cultured under control conditions and that TECS can improve the quality of those blastocysts. The increase in cell number of the mouse and human blastocysts suggests that TECS could enhance cell division of human embryos. According to published material (Cui et al., 2008, Xie et al., 2006), negative correlations between the percentage of TUNEL-positive cells and cell numbers in mouse embryos have been suggested. Therefore, although not measured, reduction of necrosis and/or apoptosis may be one explanation for the increased cell number in blastocysts obtained from TECS culture. Future experiments will confirm or refute this theory. Finally, there are advantages of the TECS in clinical use. Although the culture conditions are different in each assisted reproduction laboratory, a benefit of this system is its ability to be rapidly implemented because it can be adapted to multiple styles of culture dishes/approaches. These results of thawed mouse and human embryo development indicate that the clinical study of embryo culture using the TECS can be extended without problems. To demonstrate the clinical importance of the TECS in human embryo development, a clinical multicentre study is being prepared on human embryo development using the TECS and embryo transfer. The improved quality of developed embryos by the TECS might contribute to enhanced pregnancy rates in clinical practice. As blastocyst cell numbers were increased by the TECS, pregnancy rates resulting from embryos cultured in this system might be improved. In conclusion, the TECS enhanced blastocyst development rates of mouse embryos after the 2-cell stage and caused a significant increase of cell number in blastocysts. Thawed human embryos after the 3-cell stage tend to show an improved blastocyst development rate when cultured by the TECS. In particular, the improvements made by the TECS were significant in low-quality embryos and suboptimal culture conditions. One possible reason for the improvements could be mechanical stimuli by embryo motion based on the comparison of both mouse and human embryo development results.
Acknowledgements This study was supported by a grant-in-aid for Scientific Research on Priority Areas (No. 17076006 to K.N.) and Special Coordination Funds for Promoting Sciences and Technology from the Ministry of Education, Science, Sports, and Culture, Japan (to K.M.). References Cabrera, L.M., Heo, Y.S., Ding, J., et al., 2006. Improved blastocyst development with microfluidics and Braille pin actuator enabled dynamic culture. Fertil. Steril., S-43. Cohen, J., Simons, R.F., Edwards, R.G., et al., 1985. Pregnancies following the frozen storage of expanding human blastocysts. J In Vitro Fert. Embryo Transfer 2, 59–64. Contramaestre, A.P., Sifontes, F., Marin, R., et al., 2008. Secretion of stem cell factor and granulocyte-macrophage colony-stimulating factor by mouse embryos in culture: influence of group culture. Zygote 16, 297–301. Cui, X.S., Shen, X.H., Kim, N.H., 2008. High motility group box 1 (HMGB1) is implicated in preimplantation embryo development in the mouse. Reprod. Domest. Anim. 75, 1290–1299. Eddy, C.A., Pauerstein, C.J., 1980. Anatomy and physiology of the fallopian tube. Clin. Obstet. Gynecol. 23, 1177–1193. Fox, G.J., 2007. The Mouse in Biomedical Research, second ed. Academic Press, pp. 97–98. Gardner, D.K., Lane, M., Stevens, J., et al., 2000. Blastocyst score affects implantation and pregnancy outcome. Fertil. Steril. 73, 1155–1158. Halbert, S.A., Tam, P.Y., Blandau, R.J., 1976. Egg Transport in the rabbit oviduct: the roles of cilia and muscle. Science 191, 1052–1053. Hardy, K., Handyside, A.H., Winston, R.M.L., 1989. The human blastocyst: cell number, death and allocation during late preimplantation development in vitro. Development 107, 597–604. Kawamura, K., Fukuda, J., Kumagai, J., et al., 2005. Gonadotropin-releasing hormone I analog acts as an antiapoptotic factor in mouse blastocysts. Endocrinology 146, 4105–4116. Lyons, R.A., Saridogan, E., Djahanbakhch, O., 2006. The reproductive significance of human fallopian tube cilia. Hum. Reprod. 12, 363–372. Melin, J., Lee, A., Foygel, K., et al., 2009. In vitro embryo culture in defined sub-microliter volumes. Dev. Dyn. 238, 950–955. Mottla, G.L., Adelman, M.R., Hall, J.L., et al., 1995. Lineage tracing demonstrates that blastomeres of early cleavage-stage human pre-embryos contribute to both trophectoderm and inner cell mass. Hum. Reprod. 10, 384–391. Nagai, T., Ding, J., Moor, R.M., 1993. Effect of follicle cells and steroidogenesis on maturation and fertilization in vitro of pig oocytes. J. Exp. Zool. 266, 146–151. Staigmiller, R.B., Moor, R.M., 1984. Effect of follicle cell on the maturation and developmental competence of ovine oocytes matured outside the follicle. Gamete Res. 9, 221–229. Suarez, S.S., 1987. Sperm transport and motility in the mouse oviduct: Observation in situ. Biol. Reprod. 36, 203–210. Wang, J.H.C., Thampatty, B.P., 2006. An introductory review of cell mechanobiology. Biomech. Model. Mechanobiol. 5, 1–16. Xie, Y., Wang, Y., Zhong, W., et al., 2006. Shear stress induces preimplantation embryo death that is delayed by the zona pellucida and associated with stress-activated protein kinase mediated apoptosis. Biol. Reprod. 75, 45–55. Xie, Y., Wang, Y., Puscheck, E.E., et al., 2007. Pipetting causes shear stress and elevation of phosphorylated stress-activated protein kinase/jun kinase in preimplantation embryos. Mol. Reprod. Dev. 74, 1287–1294. Zervomanolakis, I., Ott, H.W., Hadziomerovic, D., et al., 2007. Physiology of upward transport in the human female genital tract. N.Y. Acad. Sci. 1101, 1–20. Declaration: Keiji Narusee launched the bio-venture company, Strex Inc., in 2003 and serves as a Chief Scientific Officer. The other authors report no financial or commercial conflicts of interest. Received 16 May 2009; refereed 8 June 2009; accepted 11 November 2009.
[ Full Article ]
News: Anti-depressants linked to plummeting sperm count
Heidi Nicholl 31 October 2006
Researchers at Cornell Medical Center in New York have discovered that commonly prescribed anti-depressants may have the unwanted side effect of drastically lowering male sperm count. Tests were conducted on two men over a two year period, during which time their sperm count changed from normal before taking the anti-depressants, to almost zero after taking the medicines. The sperm count of both men recovered to normal levels once use of the drugs was discontinued. [ Full Article ]
Article: Ethics and safety in the 'saviour child' debate
Juliet Tizzard 24 June 2003
This week, the British media has gone crazy about a newborn baby. His name is James Whitaker and he was conceived in order to provide stem cells for his older brother, Charlie. In the reams of commentary which followed James' arrival into the world, two main ethical issues emerged. The first question is whether it is wrong to create a child in the hope that it will be of some use to another child. The second issue, which follows from the first, is whether it is psychologically harmful to a child to know that it has been born for this purpose.
These questions raise what seem like new dilemmas brought on by the new age of genetics. But, in reality, they are rather old quandaries which many parents have faced before. Couples with a sick child whose health depends upon a matched tissue donation have been known to have another child in the hope that they will be a suitable donor. Whilst this might not be considered the most noble reason for having a child, it is usually regarded as a private family decision. And indeed it was in the case of the Whitakers, whose second child, Emily, was conceived naturally, but who sadly turned out not to be a compatible donor for Charlie. To answer the second question, whether psychological harm will be done to the so-called saviour child, one need only look at Emily, who shows no signs of being neglected or psychologically scarred in any way, despite the fact that her stem cells could not be used to treat her older brother. If parents have been left to make such judgements privately up until now, why were the Whitakers forced to have their wishes scrutinised by the nation? Because the technique they sought to use is one normally carried in order to avoid the birth of a child with an inherited disease. In the case of the Whitakers, the government regulator, the HFEA, did not consider the reason for having embryo screening to be sufficiently immediate to warrant its use. As chairman, Suzy Leather, told a number of newspapers, 'No one can say for certain what the long-term risks of embryo biopsy are. If there are benefits for the child to be created from the biopsied embryo... the balance of potential harm and potential good falls in a different place than if you're simply biopsying an embryo for the benefit of another person.' This sounds reasonable enough. But it is important that we do not get safety and morals mixed up in a case like this. If people have difficulty accepting what the Whitakers did, they have to find a way of explaining why they think that. Perhaps people who object to this case really are concerned about the slim chance that the procedure will have damaged James Whitaker in some way. But sometimes safety concerns can be an easy route out of a moral maze. Mere mention of a 'precautionary approach' is often enough to trump all other concerns. The fact that James did not himself benefit from the embryo screening procedure does make the issue slightly different, but only in the sense that it might have made it a more difficult decision for his parents. Decisions that parents make in relation to their children are often about weighing up risks and benefits and making a judgement which seeks to maximise their health and well-being. The difference with Jayson and Michelle Whitaker is that, because of their unfortunate situation, the stakes were higher. [ Full Article ]
|


 Authors:
Authors: