

IVF NewsAnnouncement: HANDS ON TRAINING IN CLINICAL EMBRYOLOGY AND ASSISTED REPRODUCTIVE TECHNOLOGY-INSTITUTE OF REPRODUCTIVE MEDICINE AND WOMEN'S HEALTH ,MADRAS MEDICAL MISSION CHENNAI INDIA
DR.THOMAS, CFC - Chennai 18 August 2007
Dr.Thomas IVF- The International School of Embryology is conducting ongoing IVF training programme for Embryologist and Gynaecologist.
Embryologist: Sperm wash methods and Intra uterine insemination (hands on experience.). IVF Lab. basics, sterile techniques, culture media, preparation of culture dishes for IVF and ICSI (with and without oil overlay), handling of oocyte under stereo zoom microscope and insemination with sperms, sperm preparation for IVF & ICSI, denuding eggs, pronuclear stage observation, sigle culture and group culture,day 3 embryo transfers, embryo transfer techniques, setting up of inverted microscope and micro manipulator system for performing ICSI, ICSI dish preparation, doing microinjection (IVF and ICSI hands-on) , advise regarding settings up of IUI and IVFlab,Laser Assisted Hatching, Sperm Freezing,Embryo freezing( 2PN& cell stage) PESA, MESA andTesticular Biopsy .....duration 1 to 2 months
Medical graduates (Gynaecologists) : infertility history taking ,patient examination , pre IVF&ICSI investigation ,tests advised patient selection criteria, various ovarian stimulation protocols (COHS), tailoring protocols as per patient needs, performing trans vaginal ultrasonography, follicular growth monitoring, Dummy Embryo Transfer, semen analysis, semen culture, adjuvant drugs used in ART, management of OHSS and oocyte retrieval (pick-up) Frozen Embryo Transfer,Egg donation and Embryo donation and surrogacy.....duration 1 to 2 months Interested candidate may contact Dr.Thomas Institute Director Dr.Thomas ivf - International school of Embryology-chennai Chennai Fertility center and Research Institute - chennai Dr.Thomas Fertility center & Hospital - Pondycherry Chennai India. Email: [email protected] or [email protected] +919841165197 [ Full Article ]  
Article: The truth about selective termination
Juliet Tizzard 11 March 2003
Over the weekend, a misleading and inflammatory story appeared in the Sunday Times newspaper concerning the number of selective terminations performed in the UK. Entitled 'IVF mothers abort 'spare' babies', the article told us that 'women who find they are expecting twins or triplets after receiving treatment for infertility are choosing to have one or more babies aborted'. Further, the article told us that babies are destroyed 'usually to spare the mothers the additional burden of raising them'. The article gave the impression that hundreds of women are destroying their unwanted multiple babies on a whim to suit their lifestyles. But the reality of selective terminations is rather different.
Selective terminations are offered to women who are carrying twins, triplets or quads; most, though not all, of which are the result of fertility treatment. Those who decide to reduce the number of fetuses that they are carrying do not do so for their own convenience, but because of the health risks to their prospective children. Babies in multiple pregnancies are more likely to be born early, thereby increasing the chance of low birth weights and increasing the chance of disability. Although the selective termination itself is not without risk to the whole pregnancy, some couples feel that such a risk is worth taking in order to promote the health of the remaining fetuses. What provoked the publication of this story? Are selective terminations on the rise or more frequently offered to women with multiple pregnancies? It seems that the story was written after new statistics on the number of abortions performed in England and Wales were released by the Office of National Statistics. The statistics show that the total number of abortions performed in 2001 was 187,402. Of these, 40 were selective terminations, 20 of which were carried out because of fetal abnormality. This very small number of selective terminations has hovered around 40 for the past decade and, if anything, is likely to fall from now on, as the number of multiple conceptions starts to come down. Contrary to the impression given by the Sunday Times article, selective terminations are not common, nor are they on the increase. They are performed in rare circumstances in which, for an individual couple, reducing the number of fetuses in a pregnancy, as undesirable as it might seem, is the best way to protect the health and wellbeing of their future children. [ Full Article ]
News: Vatican conference opposes IVF
Dr. Kirsty Horsey 08 March 2006
Pope Benedict XVI has told an international Catholic conference on the scientific and bioethical considerations of 'The Human Embryo Before Implantation', that IVF embryos have a right to life, even before implantation. Speaking to the Pontifical Academy for Life, he declared that all human life was 'sacred and inviolable' and that 'moral judgment is valid from the start of the life of an embryo, even before it is implanted in the maternal womb'. The Vatican hosted the conference to review whether current scientific data supports the Vatican's hard-line position on IVF. The Vatican opposes IVF and related procedures because embryos created in a laboratory are often discarded, whereas others are frozen and still others are created for medical research purposes, for example to create stem cells. [ Full Article ]
Article: A tilting embryo culture system increases the number of high-grade human blastocysts with high implantation competence
Reproductive BioMedicine Online 15 March 2013

PII: S1472-6483(12)00699-2 doi:10.1016/j.rbmo.2012.11.014 © 2012 Reproductive Healthcare Ltd. Published by Elsevier Inc All rights reserved. AbstractHuman embryos normally experience mechanical stimuli during development in vivo. To apply appropriate stimuli to embryos, this study group developed a tilting embryo culture system (TECS) and investigated whether it could improve the grade of fresh human embryos compared with a control static culture system. A total of 450 retrieved oocytes from 32 IVF or intracytoplasmic sperm injection cycles of 32 women were cultured for 5–6 A culture system that produces high-quality blastocysts capable of implantation is critically important for IVF and embryo transfer. Human embryos normally experience mechanical stimuli during development in vivo. To apply appropriate stimuli to embryos, we developed a tilting embryo culture system (TECS) by placing a culture dish on an automatically tilting plate to move embryos back and forth along the bottom of the dish. We investigated whether the TECS could improve the grade of fresh human embryos to be transferred compared with that of a control static culture system. A total of 450 retrieved oocytes from 32 IVF or intracytoplasmic sperm injection cycles of 32 women were cultured for 5 IntroductionThe development of a reliable culture system to increase the number of usable embryos with high implantation competence in one oocyte retrieval cycle is critically important for IVF and embryo transfer. Some reports of culture systems to control chemical and mechanical microenvironments for in-vitro mammalian embryo culture have been published, such as a microwell approach (Vajta et al., 2000, Hashimoto et al., 2009, Ebner et al., 2010), pulsative mechanical microvibration (Isachenko et al., 2010, Mizobe et al., 2010) and dynamic culture systems with fluid motion (Suh et al., 2003, Cabrera et al., 2006, Smith and Takayama, 2007, Blockeel et al., 2009, Heo et al., 2010, Smith et al., 2011, Swain and Smith, 2011). For human embryo culture, microwell culture increases the cell number of the inner cell mass in blastocysts (Hashimoto et al., 2009), and pulsative mechanical microvibration improves the pregnancy rate regardless of the day of embryo transfer (Isachenko et al., 2010). These results suggest that human embryonic development in vitro can be significantly improved by optimization of chemical and mechanical microenvironments. In vivo, human embryos are normally transported to the uterine cavity from the Fallopian tube, where fertilization and early embryogenesis occur. Phasic contraction of the smooth muscle in the wall of the Fallopian tube and the currents produced by its ciliated epithelium enable the Fallopian tube to act as a peristaltic pump to push the embryo towards the uterotubal junction (Lyons et al., 2002, Lyons et al., 2006, Zervomanolakis et al., 2007). This movement likely stimulates the embryo continuously during transport, which may also be affected by direct contact, because the tubal lumen from the ampulla to the isthmus and the diameter of an embryo are similar. Such motion and contact presumably provide mechanical stimuli, such as shear stresses, compression and frictional forces, from the tubal fluid. Mechanical stimuli can induce the proliferation and differentiation of many cell types such as endocytes, muscle cells and osteoblasts (Wang and Thampatty, 2006). Therefore, mechanical factors in the Fallopian tube might play an important role in embryonic development. However, the static culture conditions used in conventional IVF do not mimic these mechanical stimuli for embryos. In a previous study (Matsuura et al., 2010), to apply appropriate mechanical stimuli for routine clinical use, this study developed a tilting embryo culture system (TECS) by placing a conventional culture dish on an automatically tilting plate to move embryos back and forth along the bottom of the dish using mouse embryos or donated human embryos destined to be discarded. It was found that the TECS was safe for embryos and significantly increased blastocyst cell numbers under mechanical stimuli without inducing apoptosis. The current study investigates whether the TECS increases the numbers of morphologically high-grade human blastocysts for embryo transfer or cryopreservation compared with those obtained by a control static culture system. Materials and methodsPatientsThis study was approved by the Institutional Review Boards of Hiroshima Prefectural Hospital (reference no. H19-10, approved 31 August 2007) and Okayama University (reference no. 420, approved 24 April 2007). After written informed consent was obtained from patients, conventional IVF or intracytoplasmic sperm injection (ICSI) cycles were carried out in 32 women at the division of reproductive medicine, Hiroshima Prefectural Hospital from March 2008 to May 2010. Patients were enrolled when 10 or more oocyte–cumulus-complexes were retrieved. The standard infertility work up was carried out for all patients and male partners. The patient characteristics are summarized in Table 1. The exclusion criteria were women older than 40
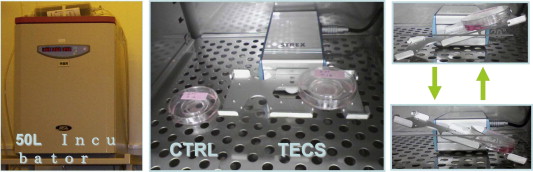
Ovarian stimulationA gonadotrophin-releasing hormone (GnRH) analogue long protocol (n Randomization of retrieved oocytesRetrieved oocytes were randomly divided into TECS and control groups. Randomization was performed using a computer-generated list of random numbers (n Tilting embryo culture systemThe TECS equipment (Strex, Osaka, Japan) was developed to apply appropriate ‘natural’ mechanical stimuli to embryos in vitro (Matsuura et al., 2010). The TECS is an electrical device with a power cord which is designed to be used in a standard humidified incubator. It consists of a control unit and a waterproof motor unit with a tilting plate (Figure 1), one-well culture dishes (IVF One Well Dish, 353653; BD Falcon, Tokyo, Japan) and/or four-well dishes (IVF MultiDish, 144444; Nunc, Roskilde, Denmark) were set on the plate. Motion parameters, such as the uniform radial velocity, maximum tilt angle and holding time at the maximum tilt angle, were set and applied by the control unit outside of the incubator. Dishes were subjected to a maximum 20° tilt in each direction at 1°/sec. This setting allowed embryos to move back and forth along the bottom of the dish at approximately 1
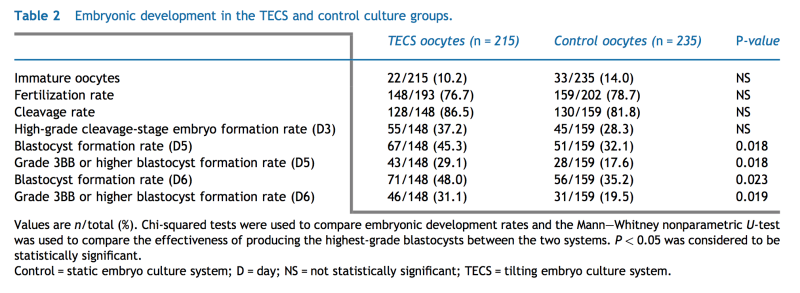
Embryo culture, cryopreservation and elective single blastocyst transferFertilization was determined to have occurred when two pronuclei were identified at approximately 20 Embryos were evaluated at day 3 in terms of the number, symmetry and granularity of the blastomeres, type and percentage of fragmentation, the presence of multinucleated blastomeres and degree of compaction, as described previously (Alikani et al., 2000). High-grade day-3 embryos were characterized by having no multinucleated cells and consisting of 7–9 cells. Furthermore, in such embryos, less than 15% of the volume of the embryo should have contained fragmentation, and the embryo should have appeared symmetrical with only slightly asymmetric blastomeres. Embryos at day 5 were evaluated using Gardner’s criteria (Gardner et al., 2000) for a blastocyst. Blastocysts scoring 3BB or higher were designated as high grade. Blastocysts containing a grade C inner cell mass or trophectoderm were not designated high grade. Morulae and blastocysts scoring less than 3BB at day 5 were cultured to day 6. The highest-grade blastocyst of each cycle, defined as the most morphologically advanced with a grade of 3BB or higher at day 5, in either group was transferred into patients at day 5 when the blastocyst was eligible for elective single blastocyst transfer according to the hospital’s policy. When the embryo grade was the same in either group, the control-cultured blastocyst was transferred. No embryos underwent assisted hatching before a fresh embryo transfer was performed. Blastocyst transfer was carried out using a Kitazato ET 3.0 Fr Catheter (Kitazato Medical, Tokyo, Japan) under transvaginal ultrasonographic guidance. Cryopreservation of supernumerary blastocysts scoring 3BB or higher at day 5 was carried out by vitrification (Kuwayama et al., 2005). All blastocysts graded 3BB or higher were vitrified if a patient was at risk of ovarian hyperstimulation syndrome or if the ovarian stimulation used the GnRH antagonist protocol, according to the hospital’s IVF/ICSI policy. When only morulae or lower-grade embryos were available, no fresh embryos were transferred. After embryos were cultured up to day 6, blastocysts scoring 3BB or higher were also cryopreserved by the same method. Conventional IVF or ICSI procedures were carried out by the same blinded embryologist. Embryos were evaluated by one embryologist who was blinded to the culture allocation, as were the clinicians, nurses and embryologists who carried out embryo transfers. Vitrified–warmed blastocyst transfer cycles and outcomes of embryo transferMicronized vaginal progesterone (450 Power analysisTo detect an increase of 15% in grade 3BB or higher blastocyst formation rate (on day 5) (i.e. from 20% to 35%) for fertilized oocytes, 137 fertilized oocytes in each group would be needed to achieve a power of 80% with a chi-squared test at a significance level of 5%. This increase in grade 3BB or higher blastocyst formation rate was based on previous results at the division of reproductive medicine, Hiroshima Prefectural Hospital during 2008 (T. Hara, unpublished results). Statistical analysisContinuous data were shown as the mean ResultsThe demographic characteristics of the couples, the type of ovarian stimulation, the result of the semen analysis and the method of insemination are summarized in Table 1. Thirty-two women were enrolled in this study. The response to ovarian stimulation was good in all patients. The mean number of retrieved oocytes was 17.0 The embryonic development rates in the TECS and control groups are summarized in Table 2. Fertilization and cleavage rates were not significantly different between groups. The rate of formation of high-grade cleavage-stage embryos at day 3 was not significantly higher in the TECS group, compared with that in the control group. The rates of blastocyst formation at days 5 and 6 from fertilized oocytes were significantly higher in the TECS group compared with those in the control group: 45.3% (67/148) versus 32.1% (51/159) (P
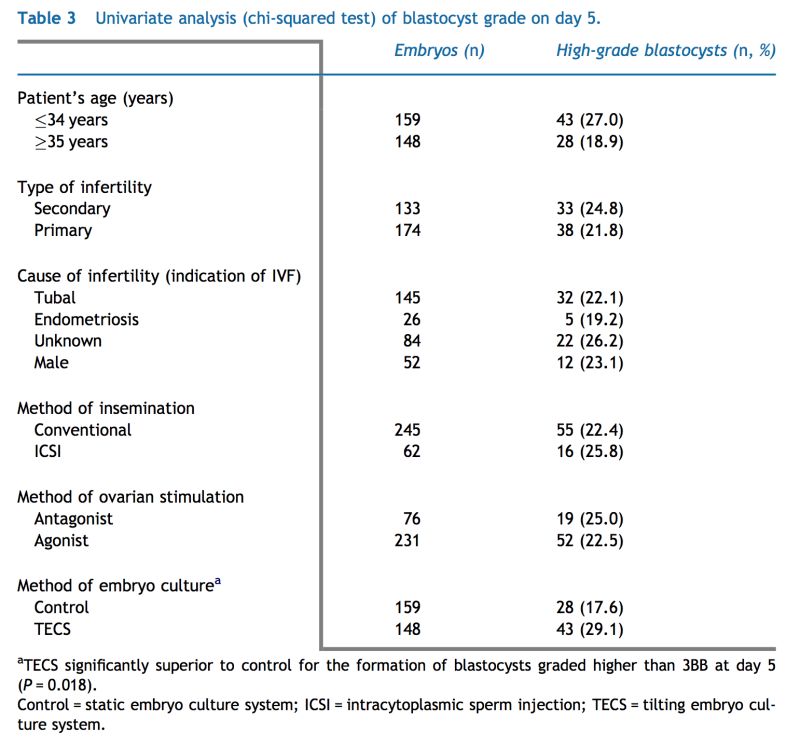
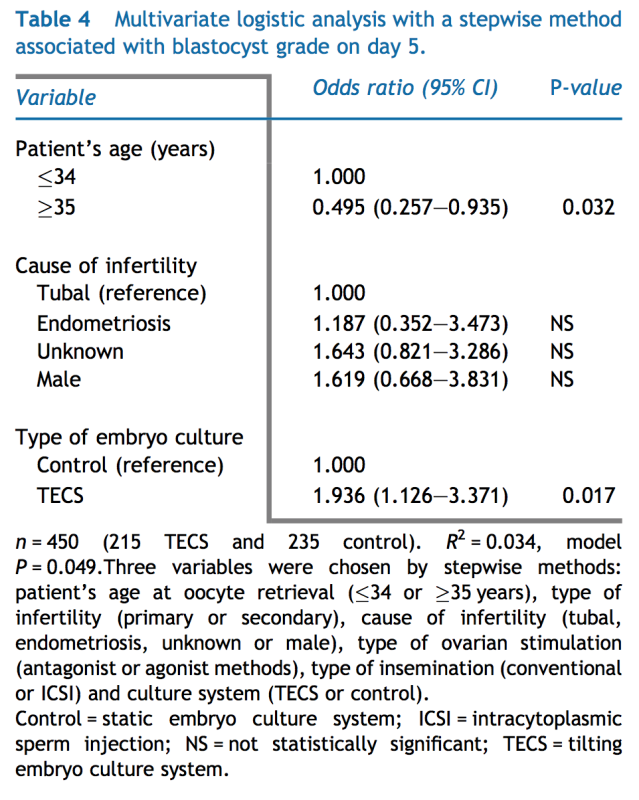
Values are n/total (%). Chi-squared tests were used to compare embryonic development rates and the Mann–Whitney nonparametric U-test was used to compare the effectiveness of producing the highest-grade blastocysts between the two systems. P Among the variables associated with embryo grade, the culture system was only related to blastocysts graded higher than 3BB at day 5, and the TECS was significantly superior to static culture (P
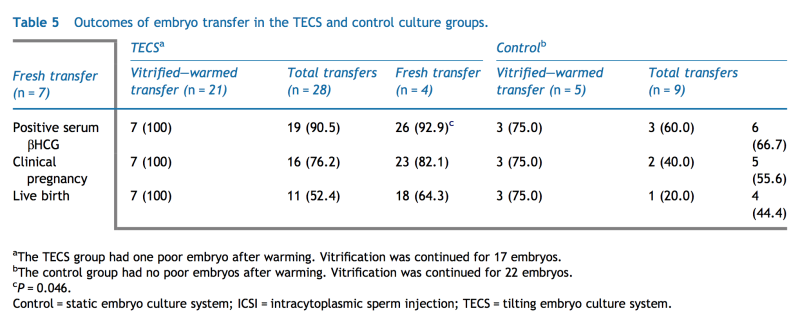
The outcomes of embryo transfer per person are shown in Supplementary Figure 1. Among 32 patients, at least one grade 3BB or higher blastocyst up to day 6 developed using the TECS or static culture for 25 patients. Among the 25 patients that received a blastocyst from the TECS or the control group, 24 patients showed positive serum βHCG, 21 became clinically pregnant and 20 had a live birth. Twenty-two babies were born because two patients delivered twice. In seven cases, either fresh embryo transfer or cryopreservation was not performed because no grade 3BB or higher blastocysts developed using either the TECS or static culture. In 11 cases, fresh embryo transfers were performed. In 13 cases, all embryos were cryopreserved to prevent ovarian hyperstimulation syndrome or because a GnRH antagonist protocol had been used. The outcomes of embryo transfer per embryo are shown in Supplementary Figure 2 and summarized in Table 5. Among the seven fresh embryo transfers from the TECS group, all embryos developed to a successful birth. The rest of the embryos in the TECS group (n
DiscussionAs far as is known, this is the first report that quantitatively defines appropriate mechanical stimulation of human embryos in vitro to improve the production of high-grade blastocysts for implantation, pregnancy and birth rates. This study confirms that the level of mechanical stimuli applied during embryo culture is not detrimental through all embryonic stages from fertilization to the blastocyst. The retrieved oocyte–cumulus-complexes from each patient were divided randomly into either a TECS or a control group before insemination or ICSI, which decreased the selection bias. The rates of formation of blastocysts graded 3BB or higher from fertilized oocytes by the TECS method were also greater than those obtained with a conventional static culture system. Thus, the TECS approach increases the number of blastocysts and would increase the cumulative number of pregnancies or live births in elective single blastocyst transfer cycles using either fresh or cryopreserved blastocysts. Thus far, the finding that a TECS enhances the grade of embryos has not been reported. There are two possible reasons for why the formation rate of higher-grade blastocysts was higher. First, in this study, the TECS was applied to oocytes before IVF or ICSI. Similar stimuli have been applied to embryos after fertilization by other institutions (personal communications: Yoshimasa Asada and Tetsunori Mukaida). The effect of mechanical stimuli on the fertilization of human oocytes remains unclear, although mechanical stimuli play fundamental roles in fertilization in other species (Knoll et al., 2003, Horner and Wolfner, 2008). In this study, the fertilization rate in the TECS group was not significantly higher than the control group. This result suggests that mechanical stimuli might enhance cell proliferation, rather than fertilization, via unknown mechanisms. Mizobe et al. (2010) reported that cytoplasmic maturation of in-vitro-matured pig oocytes is enhanced by mechanical vibration, whereas Isachenko et al., 2010, Isachenko et al., 2011 reported that the blastocyst formation rate of 2PN zygote increases by 10% using a mechanical vibration device. These reports suggest that appropriate mechanical stimuli before fertilization by the TECS used in this study might stimulate subsequent oocyte maturation as well as cell proliferation in the embryo. What needs to be clarified is the optimal time to apply the TECS during embryo culture, i.e. just after oocyte retrieval or after recognition of fertilization. Second, the blastocyst conversion rate was somewhat low in the control group of this study. The control conditions used in the study may be suboptimal and would explain the significant increase in blastocyst formation using the TECS over a suboptimal system, which may be another reason why this study has shown a positive improvement following TECS, although other studies using a TECS have not. One limitation is the ending of the study before transfer of all cryopreserved–warmed blastocysts, when a couple wished to discard their cryopreserved blastocysts. The implantation rate of blastocysts from the TECS group was significantly higher than that of blastocysts from the control group. However, the clinical pregnancy and birth rates from blastocysts obtained from the TECS group were not significantly higher than those from the control group, although the rates were higher for the TECS group than those in the control group. However, considering the difference in rates between the TECS and control groups, more power would clarify the superiority of the TECS over static culture. Such cumulative data need to be calculated after the transfer of fresh blastocysts and the transfer of all cryopreserved blastocysts. For this reason, this study could not clarify that the clinical pregnancy or birth rates from blastocysts from the TECS group were significantly higher than those from the control group. The second limitation of this study was that it enrolled only good responders to ovulation induction regimens. It is still unclear whether the TECS enhances the rate of formation of high-grade blastocysts from women who are poor responders to ovulation induction regimens. To address these important questions, a multicentre prospective randomized case-control trial is currently being prepared, which will include a broader range of patients. A culture system using microfluidic technology has been reported to enhance mouse embryonic development and pregnancy rates (Cabrera et al., 2006, Heo et al., 2010). Recently, this system has been applied to a clinical situation and reported to increase the production of high-quality human cleavage-stage embryos through a reduction of embryo fragmentation (Alegretti et al., 2011). Although this system is sophisticated and promises to improve embryonic development, the device that controls the continual pulsatile or peristaltic fluid flow is very specific and quite complex to use. In contrast, the TECS can be rapidly implemented in a laboratory, because it can be fitted to a standard incubator and adapted to different types of culture dishes. Using conventional culture dishes in this study, the formation rate of blastocysts graded 3BB or higher was significantly greater using the TECS compared with the conventional static culture system. Excessive shear stress has been reported to cause physical damage to embryos (Xie et al., 2006, Xie et al., 2007). Thus, shear stresses exceeding 1.2 Another explanation for the enhancement of cell division is facilitated diffusion of waste products from cultured embryos in the TECS. After addition of a microsphere to the centre of a 50 In conclusion, a tilting embryo culture system was developed to apply appropriate mechanical stimuli such as shear stress to embryos in vitro for clinical assisted reproduction, which leads to a higher rate of production of high-grade blastocysts with a higher implantation potential than those obtained from a static culture method. The system is a promising culture method that enhances the numbers of usable blastocysts in a single oocyte retrieval cycle by exposing them to mechanical stimuli similar to those found in the Fallopian tube. AcknowledgementsThis study was supported by a Grant-in-Aid for Scientific Research on Priority Areas to KN (‘System cell engineering by multi-scale manipulation’, no. 17076006) and Special Coordination Funds for Promoting Sciences and Technology to KM from the Japanese Ministry of Education, Science, Sports and Culture. References
[ Full Article ]
News: Effects of Infection on Sperm
ASRM 17 October 2007
Washington, DC- Sexually transmitted diseases affect male fertility on the level of physiological function as well as on a molecular genetic level. At the 63rd Annual Meeting of the American Society for Reproductive Medicine, researchers presented new studies on the impact STIs have on sperm’s DNA and on the use of assisted reproductive techniques to help HIV-discordant couples in which the male partner is positive achieve a safe pregnancy.
An international group from Spain, Mexico, and the United States found that infection with Chlamydia trachomatis and Mycoplasma sp. might contribute to reduced fertility in infected men by increasing DNA fragmentation. Antibiotic treatment to cure the infection resulted in decreased DNA fragmentation and the achievement of pregnancy for a large majority of the treated couples. Sperm DNA fragmentation in the male partners of 143 infertile couples was compared with that in a control group of 50 fertile males. The infertile men’s sperm exhibited a level of DNA fragmentation 3.2 times higher than that of the controls. Sperm concentration, motility and morphology also were impaired in the infected men. The effect of antibiotic treatment on sperm DNA fragmentation was assessed in 95 patients. After approximately four months of treatment, the patients’ sperm DNA integrity improved an average of 35.7%. During the course of treatment, 12.5% of couples achieved pregnancy, while after treatment was concluded, 85.7% of couples achieved pregnancy.�
Researchers in Monterrey, Mexico investigated the effect of HIV infection on the DNA maturation process and the integrity of sperm cells. They found that the HIV-positive patients’ sperm chromatin did not exhibit any increased incidence of alteration in�
comparison to the healthy controls’. There was also no correlation between the patients’ viral load and sperm chromatin alteration or the semen parameters of concentration, motility or morphology.�
Dr. Anne Kiessling and her colleagues have shown that HIV infection need not be a barrier to fatherhood. Over six years, from 2000 to 2006, the group evaluated semen specimens from 262 HIV-positive men. Semen specimens that tested positive for the presence of the HIV virus were discarded; specimens with undetectable viral loads were washed, frozen, and shipped to the patients’ infertility centers for use in assisted reproduction procedures After freezing two sperm specimens with an undetectable viral load, 151 couples went on to have IVF or artificial insemination. By the end of 2006, 69 pregnancies had been initiated, with 62 babies born. All of the mothers and babies tested negative for the HIV antibody.
Steven J. Ory, MD, President of the American Society for Reproductive Medicine, commented, “Assisted reproduction for patients living with HIV has been shown to be safe when the correct protocols are followed; it is very encouraging to see also that HIV does not cause damage to sperm’s DNA.”
O-12, Fernandez et al, Frequency of sperm cells with fragmented DNA in males infected with Chlamydia trachomatis and Mycoplasma sp., determined with the sperm chromatin dispersion, test.
O-49, Ayala et al, Evaluation of sperm chromatin integrity and seminal quality in HIV positive patients.
O-109, Kiessling et al, Assisted reproduction with sperm from HIV-infected men.
[ Full Article ]
News: Embryo tested for rhesus blood group
Dr. Kirsty Horsey 22 January 2005
Australian doctors have used preimplantation genetic diagnosis (PGD) to ensure that a baby shared a rhesus negative blood group with its mother. The team, based at the University of Sydney, used the technique to avoid the risk of rhesus disease, caused when the blood of a rhesus-positive baby triggers an immune reaction in its rhesus-negative mother. The doctors, who published the case in the early online edition of Human Reproduction, say it is the first report of using PGD for this purpose.
People described as rhesus-positive -around 85 per cent of the population - have a protein called the rhesus antigen on the surface of their red blood cells, which is missing from rhesus-negative individuals. During most of pregnancy, the blood of a mother and her fetus are kept separate, but during late pregnancy or labour, a few fetal blood cells can escape into the mother's circulation. In a rhesus-negative woman carrying a rhesus-positive baby, this can provoke a response from the mother's immune system, 'priming it' to attack the fetal red blood cells in subsequent rhesus-positive pregnancies. Left untreated, this process can cause severe anaemia, and sometimes death. In the vast majority of cases, rhesus disease can be prevented by injecting a rhesus-negative woman with anti-rhesus injections throughout her pregnancy. However, of 62,000 rhesus-positive babies born to rhesus-negative mothers in England and Wales each year, around 500 have blood problems, and up to 30 will die. The Australian team treated a couple whose second child had severe rhesus disease. Following PGD to select a rhesus-negative embryo, the mother gave birth to a healthy baby girl in 2003. 'A couple who have had a significantly affect pregnancy are faced with the dilemma of whether or not to attempt further pregnancies', said team leader Sean Seeho, adding that the tendency for the disease to worsen 'with each subsequent rhesus-incompatible pregnancy plays a major part in the decision'. The technique is only an option for couples in which the father is either rhesus-negative, or has inherited the rhesus-negative trait as well as the rhesus-positive trait. [ Full Article ]
News: The pioneer of IVF in India - Dr. T C Anand Kumar passes away
Dr. Rajvi Mehta 23 February 2010

Dr. T.C Anand Kumar, the pioneer of India’s first scientifically documented test tube baby, passed away on January 26, 2010 at the age of 74. A reproductive biologist of international repute, he will always be remembered for his diverse contributions to the field ranging from the role of the neuro-endocrine system in reproduction; developing the means of administering hormones via the nasal route and spear-heading the team that produced India’s first test tube baby at the ICMR’s Institute for Research in Reproduction and the KEM Hospital, Mumbai in 1986. After his retirement as the Director of the Institute for Research in Reproduction, Mumbai, he founded Hope Infertility Clinic in Bangalore in 1991 where many of the first generation of ART specialists in the country were trained and started their careers in this field. Having attained his doctorate in India, he went to Birmingham, UK to pursue his studies. Despite several job opportunities provided to him in UK, he was committed by a national spirit and returned to India to participate in the growth of science in the young nation. It was then that he started the electron microscopy laboratory at the All India Institute Medical Sciences in the 1970 which is still functional today. He continued sharing his wisdom and experience with the younger generation of scientists by serving as an advisor on many committees on the World Health Organization, Department of Science and Technology, Council of Scientific & Industrial Research, Government of India; Department of Biotechnology, Government of India and the Indian Council of Medical Research till September 2009. His work was recognized by his peers and he received the Shanti Swaroop BHatnagar Award, the highest scientific award in the country; the Sanjay Gandhi National Award, and was fellow of prestigious Indian Academy of Science; the National Academy of Medical Science (India) and fellow of the Gonville and Caius College, Cambridge. The visionary in Dr Anand Kumar was equally concerned about the welfare of his patients seeking treatment with newer reproductive technologies. When the first scientifically documented test tube baby was born, he was always questioned whether an over populated country needed test-tube babies. With this modality of treatment gaining acceptance and hundreds of clinics operating in India, he took a lead in formulating National Guidelines for Accreditation, Supervision and Regulation of ART Clinics in India. A man who stood for truth had the greatness to give away his fame and glory of being the pioneer of India’s first test tube baby when he discovered all the hand-written notes of Dr Subhas Mukerjee. Dr Mukerjee from Kolkata had claimed to have created a test tube baby in 1979 (the second in the world) but his claims were neither substantiated nor recognized by scientists or the authorities leading to the man ending his life prematurely. Dr Anand Kumar had the courage to research his predecessors’ findings and scientifically present it to the world giving Dr Mukerjee his due place in medical history (Anand Kumar T C. Curr Sci. 72:526-531; 1997). Such generosity and honesty is a very rare and precious attribute. Dr Anand Kumar’s love for science and the search for the truth will always be remembered. His students who are now highly placed all over the world would always cherish their mentor. He is survived by his wife, Karpagam son Vijay and a daughter Ambika and three grand children. [ Full Article ]
News: Lesbian couples 'could have own baby'
Dr Kirsty Horsey 20 January 2002
Scientists at the Reproductive Genetics Institute in Chicago, US, say that they have developed a technique that could be used to allow two women to have a child together, without the need for sperm.
The technique involves manipulating cells taken from a woman and turning them into 'artificial sperm' which could then be used to fertilise another woman's egg, allowing two women to be the genetic parents of a child. The technique was developed to help men with no sperm have children. The Chicago scientists say that they are already trialling the technique on human eggs, and it may be available within two years. Many other scientists, however, believe that the technique is dangerous. It involves a process known as 'haploidisation', where chromosomes within a cell are forced to separate in half. It is believed that this might cause illnesses that would not be apparent until the child was older. Professor Bill Ledger, from Sheffield University in the UK, said 'this technology has a high risk of creating damaged people and therefore I don't think it should be allowed to go ahead'. But Mohammed Taranissi, a UK fertility specialist who has been working with the Chicago team, believes that the technique shows promise. He said 'it's being done in human eggs as we speak and the first results are going to be presented at a conference in April'. [ Full Article ]
Article: In Vitro Fertilization
Conceivable World 08 December 2008

What Is In Vitro Fertilization (IVF)? [ Full Article ]
News: Do Older Women Need More Embryos?
ASRM 17 October 2007
Washington, DC – Several new research studies presented at the American Society for Reproductive Medicine meeting tackled the question of how best to help older women seeking to have children.� Using data collected by the Society for Assisted Reproductive Technology (SART) the SART writing group analyzed data from IVF cycles performed between 2000 and 2004. They examined records of more than 5500 cycles performed in women over age 37. They found that for 38 and 39 year olds, compared to a single embryo transfer, the use of up to two embryos increased the number of cycles leading to a live birth; however transferring more embryos did not increase the delivery rate, but did increase the number of multiple births. For women age 40, using 3 embryos did increase the delivery rate, but not the multiple-birth rate. For women aged 41 and 42, transferring more than 2 embryos did not increase the delivery rate, but did increase the number of twins. Another study by that same research team evaluated more than 38,000 cycles in women over age 37. They found that for 38 and 39 year old women both delivery rates and rates of multiple-birth rates increased as the number of embryos transferred increased to 3. Transferring more than 3 embryos did not increase pregnancy rates for this age group. Forty year old patients did see an increase in pregnancy rates as well as rates of multiple gestations. A team from the Robert Wood Johnson Medical School found that increasing the number of embryos transferred in patients over age 40 could increase their pregnancy rates. A team of researchers in Houston and Colorado analyzed nearly 300 cycles done on 41 and 42 year old patients in their programs. They used the outcomes of those cycles to create a mathematical model that projects that cycles using up to 6 embryos for patients over age 40 would result in very few multiple gestations. In Connecticut, insurance companies are required to offer coverage for infertility patients up to age 40. Researchers found that women beyond age 40 were treated successfully. The live birth rate for 43 year olds was 10% and for 44 year old patients it was 5.4%. “SART is committed to collecting and using data to ensure we provide our patients the best care possible. We are constantly striving to maximize the chances for each patient to have a safe successful singleton pregnancy,” said David Grainger, MD, MPH, President of the Society for Assisted Reproductive Technology (SART).
O-75, Stern et al, Optimizing the Number of Cleavage Stage Embryos to Transfer on Day 3 in Women 38 and Older: A SART Database Study
P-110, Hickman et al, Are We Justified in Transferring more Embryos in Older Women? P-515, Cetinkaya et al, Reproductive Outcome of Women > 43 Years Old Undergoing ART Treatment with their own Oocytes Pasquale Patrizio, MD contact for discussion.
[ Full Article ]
|


 Tetsuaki Hara, MD, PhD received his MD from the Hiroshima University School of Medicine in 1980. Following his residency and completion of his doctorate in 1991, he became a university instructor in 1991, assistant professor in 1996 and associate professor of gynaecology and obstetrics in 1999, at Hiroshima University School of Medicine. Since 2007, he has worked as a director of the division of reproductive medicine, Hiroshima Prefectural Hospital. Currently, his research interests include ovarian reserve, ovarian stimulation, polycystic ovary syndrome, single-embryo transfer, embryo culture and gynaecological endoscopic surgery.
Tetsuaki Hara, MD, PhD received his MD from the Hiroshima University School of Medicine in 1980. Following his residency and completion of his doctorate in 1991, he became a university instructor in 1991, assistant professor in 1996 and associate professor of gynaecology and obstetrics in 1999, at Hiroshima University School of Medicine. Since 2007, he has worked as a director of the division of reproductive medicine, Hiroshima Prefectural Hospital. Currently, his research interests include ovarian reserve, ovarian stimulation, polycystic ovary syndrome, single-embryo transfer, embryo culture and gynaecological endoscopic surgery.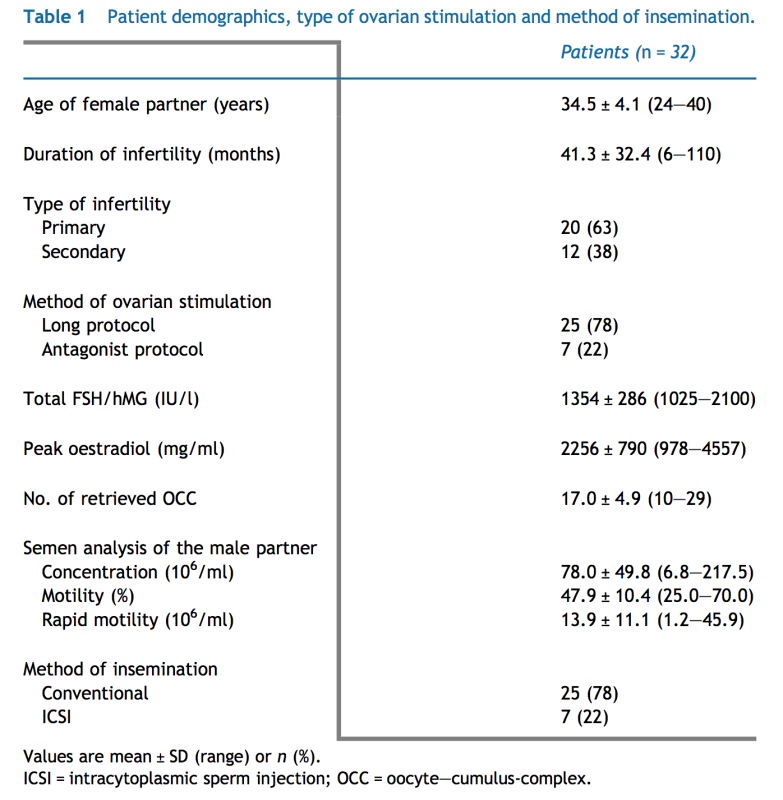
 35
35